

Causes of Tinnitus in Kids 11 through Teens

Your teen can have tinnitus without you even knowing it, because kids don’t think this is anything to worry about.
But it is: future hearing loss.
Cause of tinnitus in teens?
It’s high level exposure to music, says Rivka Strom, AuD, CCC-A, chief audiologist at Central Hearing LLC in NY.
“Whether they attend concerts without ear protection or listen to their music on their iPods/smartphone with the volume turned up to the highest, they are putting their ears at great risk for damage.”
Alarming Tinnitus Teen Study
Tinnitus was affecting a lot of kids between 11 and 17, as determined in a study of 170 kids.
A little over 54% of the kids in this study reported tinnitus in the previous 12 months.
No — Tinnitus Is NOT an “Old Person” Condition
“Ringing in the ears,” as tinnitus is often known as, is affecting more and more young people, due to our increasingly loud society.
Today’s kids and teens, perhaps more than any past generation, think that loud is cool.
- Everything just has to be as loud as possible.
- The louder the better, they believe.
- It’s as though loud is the new smoking.
Most of the study subjects reported habits that can cause hearing loss such as the use of ear buds and being in very noisy places.
Of the 54% (93 kids) who had experienced tinnitus in the prior 12 months, 51 said they experienced it after listening to loud music.
“If this teen generation continues to expose themselves to very high noise levels,” says Tanit Ganz Sanchez in the study paper (Scientific Reports, 2016), “they’ll probably suffer from hearing loss by the time they’re 30 or 40.”
Nerve cells on a structure called the cochlea can be damaged by loud noise. The cochlea is in the inner ear.
In response to damaged nerve cells, other parts of the inner ear try to take over. This causes tinnitus.
Sanchez warns that if kids and teens continue to engage in listening to loud sounds or being in loud environments, that by the time they are 25 they may have serious hearing loss.
Remember, this generation of youth is being exposed to a whole new level of noise.
So even though you, as parents, somehow made it to young adulthood without significant hearing loss, you cannot use this as a yardstick to measure how your children’s hearing is going to be by the time they’re 25.
It’s time to sit down with your adolescents and teenagers and tell them about tinnitus.
It’s funny how parents who stay on top of their kids’ dental health and vision tests are often the same parents who never give a single thought to hearing!

Dr. Strom is a member of the American Speech Language and Hearing Association and has received several awards including Brooklyn College’s Excellence In Audiology Award.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Lisa F. Young
Source: sciencedaily.com/releases/2016/07/160713101623.htm

Can You Die from an Esophageal Spasm?
An esophageal spasm can feel just like a heart attack or angina from severely clogged arteries.
The esophagus is the “food pipe” through which food and drink go down.
“Esophageal spasms can be painful,” says J. Mark Anderson, MD, DABFM, of Executive Medicine of Texas and who is board certified in family medicine.
“Some people often mistake esophageal spasm for a heart attack,” continues Dr. Anderson.
“It comes on quickly, with little warning and can be quite frightening.
“The causes of esophageal spasm can vary, from ingesting spicy or hot food, drinking alcohol, use of certain medications, excessive stress or acid reflux.”
How long can an esophageal spasm last?
A few minutes to a few hours, says mayoclinic.com.
The esophagus is made of muscle, but not the kind of muscle that’s in your biceps or legs, for instance.
But being that it’s muscle tissue, the esophagus has the potential to go into a spasm, and it can be quite painful.

Shutterstock/New Africa
Symptoms of Esophageal Spasm
• The chest pain can be intense.
• There may be a squeezing sensation.
• It’s enough to make the patient fear a heart attack in progress and prompt that person to head to the emergency room.
• Doctors cannot distinguish between the chest pain of an esophageal spasm and that of a heart attack based upon the patient’s report of the symptoms.
This is why an ER doctor will order a blood test to check for a heart attack.
• There may be difficulty swallowing liquids.
• A sensation that something is stuck in your throat.
• Regurgitation of food or beverages.
Some people get very frightened when an esophageal spasm hits—not because they fear it might be a heart attack (they may have already had extensive cardiac workups showing a normal heart), but because they think this muscle spasm might kill them.
According to mayoclinic.com, “abnormal functioning of nerves that control the muscles” that you use for swallowing seem to be a cause.
According to the mayoclinic.com section on esophageal spasms, they are not fatal. In fact, there’s not even a “complications” page for this disorder.
The fact that the pain of an esophageal spasm can mimic a heart attack is no reason to believe that such a spasm can be fatal.
Opposing Information on Another Medical Site
However, on the “Prognosis” page for esophageal spasm on the medscape.com site, it states at near the top: The mortality rate is minuscule, but the morbidity rate is high.
Below the first paragraph is a header, Mortality/morbidity. The first line states: Mortality is very rare, but morbidity can be significant.
“Morbidity” means presence of disease. Morbidity can be caused by restriction in eating (e.g., inadequate nutrients) that’s related to the condition.
The last paragraph of this subsection on the page states: Primary esophageal motility disorders rarely progress and are not known to be fatal.
The next subsection, “Complications,” states: Esophageal perforation can occur with esophageal dilatation, leading to admission to the hospital, time lost from work, and possible surgery.
Surgery can result in complications such as perforation, infection and pneumonia—three conditions that the patient can die from.
But these are secondary to the esophageal spasm, so technically, the cause of death would be complications from a surgery.
Dr. Anderson explains, “While esophageal spasms are not fatal, some underlying causes, such as cancer, can be fatal. Keep in mind that esophageal cancer is rare and not one of the common causes of esophageal spasm.”

Dr. Anderson is coauthor of the award-winning book, “Stay Young: 10 Proven Steps to Ultimate Health,” and host of the nationally syndicated Staying Young Show which goes to podcast as Staying Young Show 2.0.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources
mayoclinic.org/diseases-conditions/esophageal-spasms/basics/definition/con-20025653
mayoclinic.org/diseases-conditions/esophageal-spasms/basics/symptoms/con-20025653
emedicine.medscape.com/article/174975-overview#a2

Slow Jogging at Walking Speed Compared to Regular Jogging

How does a slow jog compare to a regular jog when it comes to fitness and calories burned? (more…)

Can a Teen GIRL’s Growth Be Stunted from Strength Training?

Girls have different bodies than boys, so it’s logical to wonder if lifting weights can stunt a teen girl’s growth.
Your teen daughter—as young as 13—may be expressing an interest in strength training—either for sports enhancement, fitness or even weight loss. (more…)

Heavy Drinking vs. Binge Drinking’s Effect on the Liver

Hey, if you think you’re giving your liver a free pass on damage because you “only” binge drink instead of daily heavy drinking, you’re so very mistaken! (more…)

What Cancers Cause Blood in the Saliva?

There’s a difference between blood in the saliva and coughing up blood.
There are 3 cancers that can cause blood to be in your saliva. You need not cough to see it.
Blood in the saliva means that if you spit (no coughing, just a voluntary spitting), you may see red.
It also means that you will invariably taste the blood.
There are a number of cancers that cause blood to appear in phlegm that is coughed up, such as lung and esophageal cancer.
Some of this blood, from a mechanical standpoint, may end up retained in your mouth—not all of it will be coughed out. So technically, you’ll have “blood in the saliva.”
But in the absence of coughing it out, here are the three cancers that may cause blood to be in your saliva:
• Mouth/Oral (includes cheeks and gums)
• Pharynx/Throat (includes tonsils, adenoids and uvula)
• Leukemia
“Blood in the mouth/saliva can be from many different sources and most probably, none of them are from cancers,” points out Daniel Vorobiof, MD, former medical oncology director of The Sandton Oncology Centre in Johannesburg, South Africa.
“However, any cancer that occurs in the mouth and is not attended to might ulcerate and stain the saliva bloody,” says Dr. Vorobiof, who also runs the “Ask the Oncologist” forum in Belong.Life, the world’s largest social network for cancer patients.
So in short, if one day you begin tasting blood in your mouth, especially if you’re a nonsmoker and nondrinker, chances are far more likely that it is not from cancer.
Risk Factors for Mouth/Oral Cancer
• Age; average age of diagnosis is 62.
• Lack of fruits and vegetables
• Genetic mutations
• Smoking cigarettes and chewing tobacco (80 percent of patients)
• Drinking (70 percent of patients are heavy drinkers)
• HPV infection (25 percent of patients)
• Immunosuppressant prescription drugs
• Unproven risk factors: mouthwash and irritation from dentures
Risk Factors for Pharynx/Throat
• Lack of fruits and vegetables
• High salt/sodium diet
• Smoking cigarettes, pipes and cigars, and chewing tobacco
• Heavy drinking
• Asbestos exposure
• HPV infection
• GERD
Risk Factors for Leukemia
• Increasing age (except for “ALL” leukemia)
• Family history
• Smoking cigarettes
• Radiation exposure (such as from power lines, atomic bomb explosion)
• Chemical exposure (e.g., pesticides, benzene)
• Previous cancer treatment in the form of chemotherapy or radiation
Remember, blood in the saliva doesn’t always mean cancer.
It also has benign causes including gingivitis, ulcers in the mouth, cut in the gum or on the tongue, recent dental work, aggressive flossing or not having flossed for a while, and nosebleed.
 Dr. Vorobiof has authored more than 100 peer reviewed articles in international medical journals.
Dr. Vorobiof has authored more than 100 peer reviewed articles in international medical journals.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/oneinchpunch
Sources:
homehealth-uk.com/mouththroatcancer/
cancer.org/cancer/acute-lymphocytic-leukemia/detection-diagnosis-staging/signs-symptoms.html
headandneckcancerguide.org/teens/cancer-basics/explore-cancer-types/throat-cancer/oropharyngeal-cancer/soft-palate-cancer/#Signs and symptoms of soft palate cancer
cancercenter.com/lung-cancer/symptoms/
cancercenter.com/oral-cancer/risk-factors/
cancercenter.com/throat-cancer/risk-factors/tab/pharyngeal-cancer-risk-factors/
cancercenter.com/leukemia/risk-factors/
md-health.com/Blood-In-Saliva.html

Twitching Index Finger from Computer Mouse Use: Solutions

If your index finger is twitching, jerking or “jumping” as a result of computer mouse use, there are causes and solutions to this annoying problem. (more…)

Slip & Fall, Hit Head Hard on Concrete: Brain Bleed Prevention

The more fit your brain is, the less likely you’ll get a brain bleed from slipping on ice and hitting your head hard on the concrete.
So the question then is, “How do we make our brain as fit as possible?”
I slipped and fell on a sheet of ice in my parents’ driveway. It happened so fast that I couldn’t react fast enough to prevent the back of my head from slamming into the concrete.
I immediately bounced back up, infuriated that this just happened, and quickly walked into the garage.
My head hit the concrete so hard that I considered the possibility of an acute subdural hematoma (brain bleed). The acute timeframe is up to three days from the incident.
Symptoms could kick in immediately or be delayed for six hours, 12, 24 or 72 hours.
Oddly enough — there was no pain. In fact, I began realizing my body and head felt as though I hadn’t even fallen, save for a little wetness on the left side of my hip and back from the ice and snow.
I was feeling quite normal, but knew that brain bleeds indeed could be delayed.
“In cases where a person seems perfectly fine after a head injury, we must keep in mind that there is a condition called lucid interval,” says Sashini Seeni, MD, a family medicine practitioner with DoctorOnCall, an online doctor and pharmacy.
“Lucid interval is the period of time when the patient seems fine after a head injury before becoming unconscious.”
My mother had blacked out due to low blood pressure several years prior in the bathroom and hit her head as she fell — on the bathtub.
It took six weeks for the brain bleed (chronic subdural hematoma) symptoms to begin presenting.
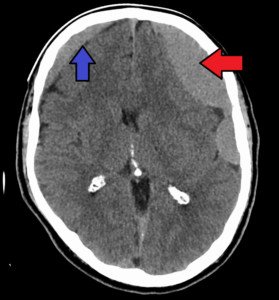
Subdural hematomas. James Heilman, MD
She was elderly. But chronic subdural hematomas (at least three weeks out from an accident) CAN occur in middle-aged people.
The subacute timeframe is between three days and three weeks out.
That very evening of my fall, the whiplash soreness – very sore — in my neck began setting in.
This really concerned me, because it suggested that my head must have really snapped back and hit the concrete hard.
However, I never developed any neurological problems (other than mild headaches on 10 separate days over a five week post-fall period).
I kept thinking of how this exact same fall would have killed an elderly person.
The primary care physician whom I saw six days post-fall told me that a brain bleed of the chronic subdural hematoma type in middle age people is exceedingly rare.
I know my head took the brunt of the fall. There had been only a few mild bruises on my left hip side.
My wrists and tailbone weren’t even affected. My butt didn’t have a single mark.
What Scared Younger Adults Who Hit Their Head Must Know
Shutterstock/Pixel-Shot
“In a patient with a head injury, the main concern is to detect intracranial hematoma, which is the collection of blood inside the skull caused by a ruptured blood vessel,” says Dr. Seeni.
“Over time, the amount of blood will increase and cause an increase in the intracranial pressure that leads to damage of the brain tissue.
“If a person does not show any immediate sign and symptoms after a head injury, look for any physical, emotional and mental changes.
“Intracranial hematoma can occur minutes or hours after a head injury.”
A chronic subdural hematoma (cSDH) is “predominantly a disease of the elderly,” says the Postgraduate Medical Journal (J 2002;78:71–75).
But if you’re middle aged or younger, and you’re worried sick that you’re going to have a brain bleed in the near future because you banged your head in the house somewhere, you need to know HOW a delayed brain bleed (cSDH) occurs in the elderly.
The Journal explains: “With aging, the mass of the brain decreases leading to an increase in the space between the brain and skull.
“This causes stretching of the bridging veins, and the greater movement of the brain within the cranium makes these veins vulnerable to trauma.”
To put this simply, when an old person gets banged in the head, there’s room for their aged, shrunken brain to shake around against the skull.
This jarring tears the veins between the brain and the skull.
The tears are very small (very slow bleeding), which is why, in a chronic SDH, symptoms take several weeks to start showing.
What about younger adults who DO die from brain bleeds?

Shutterstock/Corepics VOF
This kind of brain bleed beneath the dura mater is an “acute” subdural hematoma.
The Journal states: “Acute subdural haematomas generally occur in younger adults, after a major trauma, often associated with structural brain injury, and present within 72 hours.”
The key words here are “major trauma.”
If you, a middle age or younger adult, recently banged your head into the car door frame, or bonked your head on a table ledge after getting up from the floor … this doesn’t qualify as “major trauma.”
Other Examples of Non-Major Hits to the Head
• Accidentally walking into a closed glass door, thinking it was open (this happened to me; the glass was so clear that I proceeded to walk through and slammed my forehead).
• Banging head on anything above you when rising from the floor.
• In general, accidentally hitting your head in the course of everyday activities is non-major trauma—to the typical middle age or younger adult.
• Even falls to the ground are non-major trauma, especially if there are no rapidly developing neuro symptoms such as worsening headache, vomiting, slurred speech, confusion, sleepiness or seizures.
Examples of Major Head Trauma

Doctors evaluating an image of an acute brain bleed. Credit: Alpha Prod
Major trauma to the head occurs in vehicular accidents, being thrown from a bike or horse, skateboard and ski accidents, falling from heights, getting hit by airborne objects, and hits from contact sports.
But knocking your head into the edge of an open cupboard door isn’t quite up there with these other more major examples.
Younger and even middle aged adults have bigger brains. There’s less room for the brain to be jostled around (and tear bridging veins) from non-major hits to the head.
A bigger brain means a tighter fit against the skull.
“If a person loses consciousness, they immediately need to be treated,” says Dr. Seeni.
She urges anyone who’s hit their head hard from a fall, yet feels perfectly fine, to ask someone close to keep an eye on them.
The issue now becomes: “How do I prevent brain shrinkage?”
The less shrunk your brain is, the less likely you will get a brain bleed from minor blows to the head.
In elderly people, the hit can be trivial enough to forget about by the time the symptoms appear weeks later.
To maintain the biggest and healthiest brain possible, you need a comprehensive fitness regimen.
Work out hard, and your brain will become the best it can be.
Activity that requires balancing has been shown in studies to improve brain health. Yoga and martial arts fall under this category.
 DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Astrid Gast
Source: pmj.bmj.com/content/postgradmedj/78/916/71.full.pdf

Does Your Heart Race when Rushing Across a Room? Cause & Solution

If the only time your heart races like mad is when you hurry across a room in the house, there’s a very likely reason for this and there’s a solution. (more…)

Can Sleep Apnea Be Diagnosed While You’re Awake?



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}