

How to Tell when a Cancer Patient Is About to Die

There are ways you can tell when a cancer patient in the latest stages of disease is about to die.
These signs are an alert that death is very imminent.
“Cancer patients who are at the end of their life tend to be tired and weak, resulting in an increased requirement for sleep,” says Jonathan Stegall, MD, an integrative oncologist and medical director for The Center for Advanced Medicine, an adult cancer treatment center in Alpharetta, GA.
“They often lose the desire for food and drink, and frequently stop seeking interaction with others,” continues Dr. Stegall.
The aversion to eating even a small portion of their favorite foods is because their body, all its systems, is shutting down – and therefore has no need for any sustenance.
There will also be a reduced response to verbal stimuli.
In addition, according to a study (Hui et al), there is a reduced response to visual stimuli.
There may be a drooping of the so-called smile lines, along with grunting, hyperextension of the neck with the head tilting off the bed, eyes that do not close and pupils that do not react to changes in lighting.
These latter signs are not a 100 percent guarantee of imminent death (within three days), but the study says that very few patients who had these signs were alive more than three days later.
The study authors point out that due to the small number of subjects in this research, the results cannot be generalized to apply to illnesses other than cancer, nor to terminal cancer patients in all possible settings such as the patient’s home.
General Signs that Death Is Near for a Cancer Patient

Shutterstock/CandyBox Images
“Depending on the cancer type, pain levels can increase, resulting in a need for additional pain medication,” says Dr. Stegall.
“Breathing changes can also occur, ranging from more rapid breathing to some periods of apnea [paused breathing].
“Dying patients will sometimes become anxious, agitated and restless.
“They might see or hear things that aren’t there [or at least perceivable to family members], including loved-ones who previously died.
“Finally, patients who are close to death might lapse into a coma, where they are completely unresponsive.
“Although they are not responsive, it is believed that they continue to hear and perceive things around them.”
When a cancer patient is close to death, about to die, the process is actually pretty similar to that from other illnesses such as kidney failure, heart failure, systemic infection and COVID-19.
Whether caused by cancer or other conditions, the body shuts down pretty much the same across the board.
This is why the narrative of the dying process, that’s provided by hospice care services, is in template or general form rather than specific to a particular medical condition.
When cancer patients in movies and TV shows are shown dying (in bed), they’re typically talking and making good eye contact to a loved-one.
Then suddenly they cease talking and close their eyes, and for dramatic effect, the director has them move their head slightly away from the family member at the bedside.
In the end stage of a chronic, progressive disease (whether cancer or another illness), it certainly can happen that someone weakly speaks, then passes.
But in general, there’s a phase between their last spoken words, last open eyes – and when they take their last breath.
In acute injuries such as a stabbing or gunshot wound, a person can be talking quite a bit and then abruptly lose consciousness and die.
 Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: acsjournals.onlinelibrary.wiley.com/doi/10.1002/cncr.29602

Appearance of Pencil Stools of Colon Cancer Compared to IBS

Colon cancer can cause pencil shaped stools. So can irritable bowel syndrome.
And therein lies the problem when you see skinny poops coming out of you that resemble a pencil shape or how toothpaste looks like coming out of the tube.
Let’s take a closer look at how pencil shaped stools from irritable bowel syndrome might appear different from flattened narrow bowel movements caused by colon cancer.
“The occasional narrow stool is not of major concern,” begins Santosh Sanagapalli, MD, a consultant gastroenterologist, endoscopist and colonoscopist.
“However, a persistent narrowed stool, for example — of pencil thickness — can sometimes occur due to narrowing or obstruction of the colon from a colon cancer.
“The problem is that changes in the stool form or shape can also be a common feature of irritable bowel syndrome.”
This is caused by colon contractions or spasms.
In this case the muscles in the colon contract involuntarily. These spasms can cause changes in bowel movements.
Dietary factors, such as intolerance to certain foods or eating high-fat meals, can worsen colon contractions.
Emotional stress and anxiety are also significant contributors, as the gut-brain connection can influence bowel motility and trigger spasms.
Appearance of Skinny Bowel Movements from Colon Cancer vs. Irritable Bowel Syndrome
Dr. Sanagapalli explains, “Based on the appearance of the stool alone, one cannot differentiate between a benign cause such as IBS and a concerning cause such as bowel cancer.”
The stools from either condition will look the same as they are voided and also as they end up in the toilet bowl.
“Further, IBS is a far more common condition than colorectal cancer,” continues Dr. Sanagapalli.
What should you do?
“The decision to investigate further is based on any concurrent symptoms and the patient demographic,” says Dr. Sanagapalli.
“For example, in a young woman who describes changed (narrowed) appearance of the stool but no bleeding, weight loss, anemia or abnormal findings on examination, then the diagnosis is likely to be IBS.
“However, in an older male who describes such a change in his stool appearance, along with rectal bleeding or other concerning features such as anemia or weight loss, there would be much higher concern for colorectal cancer.
“The symptom therefore requires careful evaluation by a gastroenterologist (both history, physical examination and blood tests) to decide on the likely diagnosis and need for further investigation.”
Procedures such as colonoscopy can help visualize the colon and identify any structural or inflammatory issues, while imaging tests like CT scans or X-rays may be used to rule out other conditions.
Further investigation would likely mean a colonoscopy.
- Blood in the stools — can be red or dark
- Old blood in the stools can appear black or like a tarry substance.
- Stools that are like ribbons or pencil-thin
- A feeling of incomplete voiding after a bowel movement
- Unexplained constipation or diarrhea that persists
- Alternation between constipation and diarrhea
- Odd changes in bowel habits
- Abdominal pain or gas
- A feeling of bloating or cramping in the abdomen
- Unexplained weight loss
- Unexplained fatigue
- Unexplained back pain
 Dr. Sanagapalli is a gastroenterologist and director of the Esophageal Disorders Center at St Vincent’s Hospital, Darlinghurst. He performs diagnostic and therapeutic endoscopic procedures, and enjoys providing comprehensive and holistic care to patients with a wide variety of disorders affecting the gastrointestinal tract.
Dr. Sanagapalli is a gastroenterologist and director of the Esophageal Disorders Center at St Vincent’s Hospital, Darlinghurst. He performs diagnostic and therapeutic endoscopic procedures, and enjoys providing comprehensive and holistic care to patients with a wide variety of disorders affecting the gastrointestinal tract.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Dr. Now Scolds James K’s Enabler on “600 Pound Life”

James as a young adult
“This is mind boggling why you keep overfeeding him!” Dr. Now scolds an enabler on “My 600 Pound Life.” Finally, Dr. Now lashes out at an enabler!
The Lisa and James situation aired for the first time on March 15, 2017.
Many “600 Pound Life” viewers seethe flames at the enablers, but Lisa has got to be one of the worst enablers I’ve ever seen on this show.
I thought Penny Saeger’s enabling husband was the worst, but Lisa takes the cake (no pun intended).
The subject is James, 46 (as of 2017), who’s confined to his bed and has grotesque pebble-like protrusions, lesions and other yucky stuff on his legs from cellulitis that is prone to draining.
I don’t mean to be cruel, but in all sincerity, James’ lower body looks like Jabba the Hutt’s.
Lisa doesn’t seem to mind wiping up the oozing every day nor having pulled their teen daughter out of school to help care for her father.
Because James is paralyzed by his weight, he is 100 percent dependent on Lisa for food intake, and she is shown bringing him plate after plate loaded with high calorie food.
About an hour into the two hour episode, Dr. Now really lays into her after James not only fails to lose the recommended amount of weight to qualify for the surgery, but he gains some.
• Dr. Now’s voice is deeper and more snarling.
• He’s not the softie he usually is.
• He corners Lisa by asking what would happen if she just stopped bringing him all the food.
• She replies, “I will have hell to pay for the rest of the day.”
• Dr. Now fires back something like, “What’s he gonna do to you while he lies in bed? Scream and yell? So let him scream and yell!”
Later on in the show, James is given yet another chance by Dr. Nowzaradan, and when he comes back for his next weigh-in, he’s UP by 158 pounds – after Lisa insisted that she kept James on the prescribed diet.
That’s when Dr. Now chastises Lisa: “This is mind boggling that you keep overfeeding him.”
And he’s so right: It is mind boggling how these enablers operate. Even after James suffered acute heart failure, that wasn’t enough for Lisa to stop bringing him platefuls of food. Every time he went back for a weigh-in, he had gained.
So Lisa, as well as other enablers, believe they will have hell to pay for the rest of the day should they refrain from overfeeding their 600-pound-plus significant others, grown kids or parents.
What is this “hell” when compared to the hell of playing a key role in CAUSING THEIR DEATH?
Are these enablers so thin skinned that they can’t ignore a temper tantrum that’s being thrown from the confines of a BED?
It was very refreshing to finally see Dr. Nowzaradan scold an enabler. He needs to go into scolding mold more often, even if it doesn’t snap the enabler out of their delusion.
But I’m betting that more times than not, it would. It’s just that in the James and Lisa case, it didn’t.
After 11 months, James and Lisa were finally turned away by Dr. Now, though the doctor had supported the idea of having two physical therapists drop by and help James sit up for the first time in a few years.
At the end James announced that he was determined to get under 600 pounds and get the surgery, but the only way this will ever happen is if Lisa stops being his enabler.
“My 600 Pound Life” takes the viewers back in time to the childhood of every subject, so that we can see what could have triggered the descent into 600 pound madness.
I’d like to see some of the footage that’s spent on boring travel preparation scenes be replaced by even just five minutes of exploring the childhood of the enabler.
Lisa is slowly killing her daughter’s father and enlisting in her help to do so. Sure, James could always say “No” to all the eating, but he can’t get any food without his enabler’s help.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

How to Beat Menopausal Blues by Lifting Heavy Weights
The depression of menopause can swoop in like a vulture, but you can fight back by learning to lift heavy things!
Chase away the menopause blues by training your body to lift and carry heavy weights. (more…)

How to Do Seated Hamstring Curls to Burn the Most Fat

There is a way to do seated hamstring curls to burn the most fat.
Seated hamstring curls may seem simple enough, but there are specific things you can do to maximize your fat burning results.
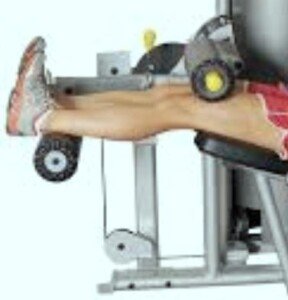
With seated hamstring curls, make sure your feet are always held in a 90 degree angle. Do not let them relax, as shown below.
From the moment you begin pushing down on the pad, all the way throughout pushing the pad to the down position (fully flexed knees), the feet stay in a 90 degree angle.
When pressing pad down, flex knees (bend legs) as far in as possible, all the way, till you feel pad making contact with machine.
Few people do this, and instead, do seated hamstring curls only 80 or 90 percent of the way.
Depending on the make and model of the seated hamstring curl machine, the maximum knee flexion angle won’t be that much less than 90 degrees.
Other seated hamstring curl machines can be adjusted to permit quite a bit of knee flexion. At any rate, bend your legs as much as the machine will allow.
Next, hold this maximal bent position for three seconds before releasing.
In order to do this for 8-12 repetitions, you will need a lighter weight, rather than the weight you normally use. I don’t recommend this three second hold for every set, but for two or three of them.
Make sure it’s a true solid three second hold, maintaining contact between pad and machine.
When releasing the pad for seated hamstring curls, don’t let it fly up. Release with control, and bring it back down before it goes up all the way.
Legs may be as far apart as possible, closer together, or completely together for any given set.
I recommend taking all positions throughout your seated hamstring curl routine for best fat burning.
Furthermore, feet should be turned outward as much as possible, legs apart as far as possible, for at least two sets. Try this tweaking; you’ll feel the difference and will burn more fat.
For seated hamstring curls, you can lean back in the seat, or lean forward. Always make sure the support pad is secure atop your thighs. Hands can be anywhere.
Start out with a few lighter sets with the three second hold, then use heavier weight with each set (the three second hold won’t be possible at heavier weights).
Get in at least three super heavy sets in which you can move the weight only 7-10 times max — all the way back, making the pad touch the machine every time.
Make these adjustments with your hamstring curl routine for best fat burning results, and the backs of your legs will become significantly stronger and tighter.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/ESB Professional

Hamstring Curls Lying Down: Proper Techniques for Best Results

There are a few ways you can tweak the way you do hamstring curls, that will yield better and faster results, be they fat burning, stronger legs or rock-hard hams. (more…)
Exercises with No Equipment that Work Best for Overweight Teen Girls?

If you’re a teen girl trying to lose weight, you’ll get the best results from these exercise routines–even if you think you’ve inherited “big genes.”
No equipment is needed. (more…)

If Cannabis Cures Cancer, Why Do Pot Smokers Get Cancer ?

Many cancer patients use “medical marijuana” to treat pain but die of cancer anyways.
And if weed can cure cancer, you’d think that daily pot smokers would never get the disease – even recreational users. (more…)
Why Does Hair Grow in Thicker After Chemotherapy?

Many women report that their hair grows in thicker and fuller after losing it from chemotherapy.
Is this an illusion or is the hair shaft actually bigger in diameter? (more…)
My Estranged Sister Didn’t Tell Me She Had Breast Cancer
Does a woman who hates her sister owe it to her to reveal a breast cancer diagnosis, since family history is a major risk factor for this disease?
• What is the right thing to do?
• Or to put it another way, the Christian thing to do?
• What is the moral thing to do?
Would it be to withhold the breast cancer diagnosis from the estranged sister?
Assume that withholding the news has NOTHING to do with fearing that the estranged sister will blab it to the whole world.
Assume that the woman with breast cancer won’t tell her estranged sister because, at a minimum, she just doesn’t care for her sibling.
It would be honorable to put aside the hate and hostility, if it’s actually to that degree, and just tell her.
This way she knows she now has an added risk factor, and it may influence her breast cancer surveillance program.
But what if a woman tells three siblings, none of whom she’s ever been close to, at the time of diagnosis, but then doesn’t tell the fourth sibling — a woman — until 13 months later?
This actually happened to me.
My sister and I have never been friends. However, she was never friends with the other three siblings, either. Not all families operate like “The Waltons” or “The Brady Bunch.”
So why was I the “odd man” out?
Some Facts to Consider
I would have understood my estranged sister’s decision not to reveal her breast cancer diagnosis had she ALSO kept it from the three other siblings. That would have made perfect sense.
A breast cancer patient does not have to tell ANYONE.
But I can’t say this enough: There is no rhyme and reason in leaving one sibling out when you’re not friends with the other three either! That’s the kink in the chain!
In fact, she seems to contact the oldest brother (who’s very wealthy) only when she wants money.
She was in contact with the second brother for a number of years ONLY because he lived nearby her, and it wasn’t close. It was more of a familial-based obligatory thing: invite him over on major holidays.
When he moved out of her state, the contact stopped – ON BOTH ENDS. He now lives near me and our parents. The other two siblings have always lived far from her and our parents.
She has never been in regular contact with the other sister, and they couldn’t be further apart in personality.
Among my two sisters and these two brothers (there’s a third), it’s very accurate to state that there is NO relationship, no cheery and chummy camaraderie, nada, zero, nothing.
And it’s the same with me and this particular sister as well. So why didn’t she tell me of the breast cancer diagnosis? This is why I’m livid.
Tell Two Brothers of a Breast Cancer Diagnosis but Not Both Sisters?
So after I received my sister’s snail mail telling me of this shocking news – 13 months after the diagnosis – I fired back an e-mail calling her on why I was left out of the revelation early on, when she told the three other siblings.
Before you chastise me for not being more sympathetic and instead focusing it more on myself and hence sounding selfish, let me say that the tone of her letter was actually quite high-spirited, including telling me, “Cancer picked the wrong girl.” She said, “I’m doing great!” She expressed no fear of recurrence.
She obviously didn’t need my sympathy. She never even minded the hair loss, though she wore a wig and even prefers to continue wearing it for the convenience despite hair regrowth.
So yes, I felt justified in asking why three siblings were notified early on, including two MEN, when no warm and fuzzy relationship has ever existed with them.
My second brother and I are occasionally over our parents’ house at the same time.
My sister answered that she and my brother feared that I’d “slip” the alarming news to my mother by accident.
I don’t buy this. My brother has always known that I’m the last person to reveal troubling news to our elderly mother, who’s prone to excessively worrying about her kids.
I even once chastised him for telling her he had no medical insurance. When he mildly sprained a knee weightlifting, I warned him not to tell her EVEN THAT.
When I sprained an ankle a few years ago, I warned the third brother — who still does not know of the breast cancer diagnosis — not to tell our mother!
I also admonished this third brother for causing my mother endless sleepless nights — he had told her he lost his job! He could have easily concealed this, as he was living out of state at the time.
So the idea that I come across as someone who might “slip” such devastating news to our mother is totally freaking not believable.
I then asked my second brother about this exclusion. Here’s his explanation:
- Suppose I was told of the breast cancer diagnosis along with this brother.
- Sooner or later we’d subsequently be at our parents’ house at the same time.
- We then might start talking about the diagnosis.
- My mother might then overhear.
Do you buy that? I sure as hell didn’t, especially since my mother’s hearing is bad!
Everyone knows you can carry on a soft conversation in the same room as her and not be understood!
Besides, if a woman has only ONE sibling to reveal the diagnosis to, out of genuine fear of it getting overheard, don’t you think she should have told only the SISTER?
After all, whose risk of breast cancer soars with a family history: a man’s or a woman’s?
So what would I have done differently had I been told at the get-go?
I would have had a seven-month lead on serial ultrasound screenings (I also have dense breasts and began the serial screenings about six months before my sister’s revelation).
And the honest truth is, I would NEVER have “slipped” the information, and now that I know that my estranged sister was diagnosed with breast cancer, I have NO plans whatsoever of telling our parents.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}