

Can a 24/7 Headache for Several Months Be a Brain Tumor ?

Your fear of a brain tumor is not imaginary if you’ve been having a 24/7 headache for the past several months.
“The most common symptoms of brain tumors are headaches,” says neurosurgeon Charles Park, MD, Director of The Minimally Invasive Brain and Spine Center at Mercy Medical Center in Baltimore.
Can a headache that goes on 24 hours a day, seven days a week, for several months ongoing, be caused by a brain tumor?
“It is very possible that the headache can be 24/7 and last several months,” says Dr. Park.
Can you dismiss the possibility of a brain tumor if this 24/7 headache is not accompanied by other symptoms suggestive of cancer?
No. You may have heard or read something like, “If it was a brain tumor, you’d have other symptoms.”
However, that needs qualification. If the situation is not treated, you WILL eventually begin developing other symptoms.
But what about, say, three months out from the onset of the new headaches?
Dr. Park says, “At times, there can be new-onset symptoms, such as seizures, weakness and balance problems, depending on the location of the tumors.”
So during that several months, you may NOT have these signs and just have the headaches.
There are benign causes of a 24/7 headache that goes on for weeks and weeks.
One such cause is a pinched or compressed nerve that branches out of the cervical (neck) vertebrae.
A tip-off that the constant daily headache might be from a brain tumor is when the headache is the worst.
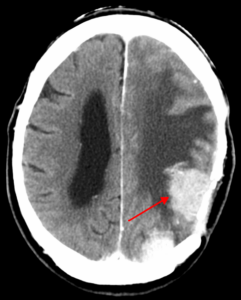
A benign brain tumor, such as a meningioma, can also cause very severe headaches. James Heilman, MD, CreativeCommons
“The classic features of brain tumor related headaches are the morning headaches,” says Dr. Park.
“When we lay down to sleep, the brain tissue, including the tumors, will expand slightly and increase symptoms, such as headaches.”
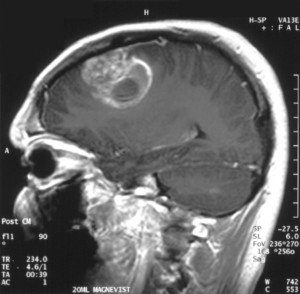
Brain tumor near top of head. Credit: Christaras
Usually, if you’ve had a constant headache every day for many weeks, that is caused by a brain tumor, there will be other symptoms with it.
Additional Symptoms of a Brain Tumor
(no particular order)
• Nausea/vomiting
• Appetite loss
• Unexplained weight loss
• Visual disturbances
• One drooping eyelid
• One eye bulging a little more than the other
• One eye a bit off center
• Hearing loss
• Cognitive changes
• Behavioral changes
• Numbness in part of the face
• Unexplained fatigue
• Speech difficulty
Symptoms may develop gradually. But a headache is often the first symptoms and the only symptom for several weeks – even several months.
It may come and go. The headache may be present only in the morning. If it’s 24/7, the brain tumor headache will very likely be at its worst on most mornings.

Dr. Park specializes in minimally invasive surgical techniques for treatment of conditions affecting the brain and spine. He’s skilled in advanced procedures and techniques that utilize innovative computer technology and image-guided surgery systems.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia

Periomenopause, Anxiety and Sadness: Treatments

Anxiety really CAN be caused by periomenopause – the precursor to menopause that no woman looks forward to. Here are natural (and surprising) treatments. (more…)

When Menopause Raises “Bad” Cholesterol: Solution
The so-called bad cholesterol can be raised by menopause—and that’s really bad.
But there IS something you can do to knock this cholesterol back down. (more…)

Does Heavy Bleeding During Menopause Mean Cancer?

Heavy bleeding during menopause is NOT normal under any circumstances and could actually mean cancer. Certain cancers can cause heavy bleeding. (more…)

Heavy Bleeding after a Colposcopy: Causes & What to Do

“It is normal after a colposcopy with a biopsy to have a small amount of spotting or light bleeding,” explains Lindsay Appel, MD, an OB-GYN with the Family Childbirth & Children’s Center at Mercy Medical Center in Baltimore. (more…)

Can Perimenopause or Menopause Cause Muscles to Twitch?

There may be a logical explanation for why perimenopause or menopause is linked to twitching muscles, but it’s probably not what you think.
Have you noticed lately that your new-onset muscle twitching seems to have coincided with your entrance into “peri” or menopause? (more…)

Can Menopause Cause Armpit Odor to Change & Get Really Bad ?

We’re not talking about a change in armpit odor strength from increased menopausal perspiration, but an actual change in the odor itself – a really stinky pungent scent.
Have you experienced the following?
• You’re in menopause or have completed it.
• You’ve had hot flashes all along—prior to the beginning of menopause, during and afterward.
• The hot flashes have intensified and you can get pretty doggone sweaty at times.
• And somewhere along the way you’ve begun noticing a DIFFERENT odor to your underarms. And it’s bad.
• This change in odor under your arms correlates to perspiration: The heavier you perspire (whether it’s from a hot flash or exercising), the stronger this new, different odor becomes.
• It’s nothing like the “usual” armpit odor you’ve always been familiar with and that you’ve certainly detected on other sweaty people.
• You may even describe this changed armpit stink as pungent. It’s very strong and unpleasant, unfamiliar to you – and you’re unnerved about it.
• You may even begin wondering if this isn’t related to menopause and instead might be a sign of some kind of cancer.
“In theory, sweating and body odor is in part related to release of certain hormones called androgens,” says Lindsay Appel, MD, an OB-GYN with the Family Childbirth & Children’s Center at Mercy Medical Center in Baltimore.
“Androgen production does change after menopause (it usually decreases), so any changes in body odor could be related to a decrease in androgen hormones in the body,” says Dr. Appel.
I’ve scoured the Internet for an answer to the title question, and all I’ve come up with is how an increase in perspiration, due to menopausal hot flashes, will cause an increase in odor or a more noticeable odor.
But this isn’t about a stronger version of the underarm odor you’ve always been familiar with or an increase in frequency of that smell.
It’s about a different, new smell, a changed odor—a new kid on the block.
And it doesn’t always come with hot flashes—but sweating from exercise brings it out.
Don’t worry, it will eventually subside as your body readjusts to the changes of menopause.
And even though the stink occurs during sweaty exercise, this new, malodorous smell is still most likely being generated from the hormonal changes of menopause.
Maybe you’ve read somewhere that liver cancer can cause a body odor and are now freaking out that you have liver cancer.
Yes, liver cancer can cause a new odor about the body.
But in the meantime, don’t sweat the menopausal stink of your armpits. Just be sure to clean them daily with soap and use an effective deodorant.
 Dr. Appel addresses a full range of obstetric and gynecologic needs for women. She has participated in several OBGYN research presentations at professional conferences.
Dr. Appel addresses a full range of obstetric and gynecologic needs for women. She has participated in several OBGYN research presentations at professional conferences.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Lipik Stock Media

Can a Woman Make Her Breasts Less Dense with Diet or Exercise?

Dense breasts are a risk factor for breast cancer.
In fact, it’s one of the higher risk factors for this disease when the density level is considered to be extremely and even heterogeneously dense.
A woman with dense breasts is four to six times more likely to get cancer when compared to a woman with the so-called fatty breasts.
Dense breast tissue is more prevalent in younger women.
And this is why mammograms are not encouraged for women of average risk who are under the age of 40.
As women age, breast tissue tends to lose its density. About 10 percent of all women have what would be considered dense breasts.
Is there anything a woman can do to make them LESS dense?
Unfortunately, there’s nothing she can do. There is no diet, no supplement, no yoga pose, no type of strength training, no aerobic activity, no pills, shots or drugs – nothing – nothing can change what nature gave her.
“The density of breast tissue usually becomes an issue when undergoing screening for breast cancer, as dense breast tissue can make it difficult to interpret mammogram imaging,” says Lindsay Appel, MD, an OB-GYN with the Family Childbirth & Children’s Center at Mercy Medical Center in Baltimore.
Dr. Appel continues, “Dense breast tissue is made up of connective tissue, blood vessels and ducts. Other tissue in the breast is fat tissue.
“It is more common to have dense breast tissue when women are premenopausal. Exposure to estrogen, like taking birth control pills, can also increase breast density.”
However, there are women with heterogeneously and even extremely dense breasts who have never taken birth control pills or estrogen treatments.
And there are many women with nearly all-fatty breasts who’ve taken birth control pills.
In general, the composition of breast tissue is the cards that a woman was dealt with at conception—her genetic blueprint.
With all that said, you should find out from the radiologist who reads your mammograms what your density level is. There are four categories:
• Fatty
• Scattered density
• Heterogeneously dense
• Extremely dense
Do you know about tomosynthesis?
This is a 3D mammogram. It “sees” things better than does a 2D (the more conventional) mammogram.
Look at it this way: Imagine that you’re standing outside a forest, trying with your eyes to locate a bird’s nest inside of it. That’s a 2D mammogram.
Now imagine that you’re hovering above the forest, an aerial view as you move around, and you’re looking down in search of that bird’s nest. That’s tomosynthesis.
While there is nothing a woman can do to make her breasts less dense, what she CAN do is take measures to live a healthy lifestyle to reduce the risk of cancer, which includes structured exercise sessions and sticking to a plant-based diet.
Dr. Appel addresses a full range of obstetric and gynecologic needs for women. She has participated in several OBGYN research presentations at professional conferences.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ESB Professional

Does Having a Big Stomach Make You Bench Press Better?

Why is it that the strongest bench pressers at the gym have big stomachs?
Does a big belly really improve one’s ability to bench press? (more…)

Should You Check for Melanoma if You Have Only a Few Moles ?

If you have only a few moles, this doesn’t mean you can blow these off & think you’ll never get melanoma.
Even if you have ONE small mole, it can still turn into melanoma. (more…)


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}