

Are Jerking Limbs Before Falling Asleep a Brain Tumor Sign ?
Have you been troubled lately by brain tumor fears because as you fall asleep, your limbs jerk?
A brain tumor can definitely cause the body to jerk in different places, but we need to define “jerking limbs” here.
There are what is known as benign myoclonus and what can be termed as brain tumor jerks.
“These are two very different entities,” says David Poulad, MD, a board certified neurosurgeon with IGEA Brain & Spine who practices in Union, NJ, whose special interests include the surgical treatment of brain tumors.
“Benign myoclonus as the name suggests is a benign condition that is not uncommon, whereas ‘jerks’ caused by a brain tumor are often a sign of seizure activity,” explains Dr. Poulad.
“It is very common for people to exhibit myoclonic jerks just before falling asleep.
“These jerks do not signal a pathologic condition and are normal in most people.”
Those who strongly believe in the paranormal have been known to insist that a sleep-related myoclonic jerk is a person’s astral body either trying to exit the physical body or making a re-entry into it!
Either way, the so-called myoclonus that occurs as you’re falling asleep is harmless.

Andrew Coop/Unsplash
It’s characterized by a single limb suddenly “jerking” or exhibiting a brief and aimless muscle contraction – enough to cause movement of part of the limb – and enough to awaken you.
Since you are now awakened and possibly startled by it, you’re too awake for this type of spasm to occur again.
But as you fall back asleep, it may indeed occur again.
The jerking of part of your leg, arm or shoulder usually occurs just once by the time it awakens a person, after which the limb returns to rest.
It is not a sewing-machine-like shaking, like you’ve certainly seen on TV when a character has a seizure on a gurney.
“The mycologic activity that occurs before sleep is self-limited, and there are no lingering after-effects that can be seen with myoclonic jerks associated with a seizure that may result in temporary paralysis or confusion,” says Dr. Poulad.
If you’re “jerking” due to a seizure from a brain tumor, this will not be a single spasm, but rather, resemble a seizure to anyone who’s observing it. It will look like shaking or tremoring.
Furthermore, if you’re having a seizure, you will not be conscious. If a sudden jerk of a limb awakens you, this was not a seizure.
A brain tumor seizure originates in the brain. The electro-chemical nerve impulses are generated in the motor control region of the brain, travel down the spinal cord and fire the muscle fibers – while the person is unconscious.
In benign myoclonus, or the “falling asleep jerking,” the electrical activity originates in the muscle fibers.
Scared Sh**tless of a Brain Tumor

Now here’s what may have triggered your fear that the falling-asleep kind of myoclonus — in which a limb jerks — might be caused by a brain tumor:
The term “myoclonus” doesn’t just mean the involuntary limb movements as you drift off to sleep.
This medical term can also mean involuntary muscle contractions from a brain tumor.
But when “myoclonus” refers to a brain tumor symptom, it does NOT refer to the sudden, one-at-a-time muscle contractions that startle you out of your semi-sleep state! Rather, it refers to a seizure.
The word “myoclonus” literally means muscle contraction. That is a VERY BROAD term.
It’s often indiscriminately used to refer to the harmless limb jerking as we fall asleep, even though “clonus” is a term that can refer to a sign of a neurological disease.
“Myoclonic jerking” is a broad term. The type seen in multiple sclerosis, for instance, does not at all resemble the type seen in a healthy person who is falling asleep.
So shouldn’t the benign sleep-related myoclonus have an official name? Yes. It’s “sleep myoclonus.”
A brain tumor can cause a seizure — which to an observer may look like jerking—at any time, including when a person is drifting off to sleep.
But again, the person will not be conscious during the seizure and will not even realize they had one if they were asleep when it occurred.

Dr. Poulad’s clinical interests involve the surgical treatment of brain and spinal cord tumors, radiosurgery, pituitary surgery, functional neurosurgery for pain and movement disorders, and minimally invasive spine surgery.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Hellerhoff
Source: ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Myoclonus-Fact-Sheet

Can a Brain Tumor Cause Twitching Muscles and Fasciculations?

Here’s an agonizing question: Would you rather your twitching muscles be caused by a brain tumor or by ALS?
Certainly you’d choose the brain tumor as a cause of muscle twitching, as this condition is not always diagnosed as terminal.
There are people out there who, over 20 years ago, were diagnosed with a brain tumor – even 30 years ago.
Several malignant masses. Credit: Jmarchn
However, there are also people – perhaps you yourself – who have somehow come to believe that a brain tumor can cause muscles to twitch.
The term “twitching” can be interpreted in different ways.
For the purpose of this article, the twitching refers to the kind of creepy-crawly sensation, or squiggling sensation, that you may feel in a muscle.
Or to put it another way, imagine the type of twitching that occurs in your eyelid happening in a larger muscle such as a hamstring, calf, arch of the foot or bicep.
So we’re not talking about trembling, tremoring, shaking or the kind of jerking that you may experience when you’re on the verge of falling asleep at night.
CAN a brain tumor, then, cause the type of muscle twitching that is commonly experienced by millions of people?
“Brain tumors can cause seizures that can even manifest as very small twitching of an extremity that can also be associated with numbness/tingling,” explains David Poulad, MD, a board certified neurosurgeon with IGEA Brain & Spine who practices in Union, NJ, whose special interests include the surgical treatment of brain tumors.
Dr. Poulad also says, “More commonly, little fasciculations in the muscle are due to electrolyte imbalances, overuse or simple fatigue.
“More commonly fibrillations/fasciculations in the muscle are due to either direct muscle injury or peripheral nerve injury and may indicate re-innervation.”
There are less serious causes of the dual symptoms of twitching muscles and numbness/tingling, and when these two symptoms seem to occur alongside each other, this doesn’t mean that they have a singular cause.
For example, carpal tunnel syndrome, a pinched nerve in the neck and low thyroid can cause a numbness and/or tingling in the fingers and fingertips.
But by chance, a benign twitching can also occur in a finger – perhaps one that’s been overused lately on the computer mouse.
“Re-innervation” simply means that the muscle cells are receiving some random electrical instructions to contract.
The “twitching” that a brain tumor might cause in a leg, for example, will not feel the same as the benign twitching you may have felt there dozens of times in the past after exercise or heavy physical activity or for no known reason.
Dr. Poulad’s clinical interests involve the surgical treatment of brain and spinal cord tumors, radiosurgery, pituitary surgery, functional neurosurgery for pain and movement disorders, and minimally invasive spine surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Can a Brain Tumor Cause a Headache in Same Spot Daily ?

Are you worried a headache that you’ve been getting in the same spot every day, fearing that it could be a brain tumor?
The bad news is that IS possible for a brain tumor to cause a headache every day in the same area of your head.
Suppose a person is having a headache – a new-onset pain – on a daily basis that’s occurring in the same spot. Can this be a sign of a brain tumor?
“Not necessarily,” says David Poulad, MD, a board certified neurosurgeon with IGEA Brain & Spine who practices in Union, NJ, whose special interests include the surgical treatment of brain tumors.
Dr. Poulad continues, “It all depends on what is the cause of the headache.
“If it is indeed due to a tumor, other symptoms will depend on where the tumor is located in the brain (i.e., is it near eloquent cortex to cause other symptoms besides headache).”
If cancer is the cause, you will more likely than not have these other symptoms.
So if it’s near the eloquent cortex you may also be suffering from minor paralysis or speech problems.
In summary, a headache in the same spot every day can have causes other than a brain tumor, but cancer actually can be a cause.
If a brain tumor is indeed the cause of a daily headache in the same area, what makes this happen?
Dr. Poulad says “regional mass effect” will “exert on the surrounding brain in that one location.”
What is “mass effect”?
When there is fluid buildup (the mass in this case) in the brain, it pushes against the organ, causing pressure – leading to the headache.
This fluid buildup, of course, would be in the same place every day (and increasing if not treated).
Sometimes the fluid buildup shifts the brain off center, and this is visible on an MRI or CT scan. When this happens it’s called a midline shift.
Bleeding in the brain can also cause a mass effect and midline shift.
But Dr. Poulad also explains that “brain tumors are not the primary cause of headaches [even daily in the same location], and it would be more likely that the patient has some form of migraine or headache syndrome.”
Do not panic if a doctor orders an MRI or CT scan of your head.
Dr. Poulad’s clinical interests involve the surgical treatment of brain and spinal cord tumors, radiosurgery, pituitary surgery, functional neurosurgery for pain and movement disorders, and minimally invasive spine surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Can a Brain Tumor Cause Twitching Muscles and Fasciculations?
Brain Tumor Can Cause Smelling Something Bad that’s Not There
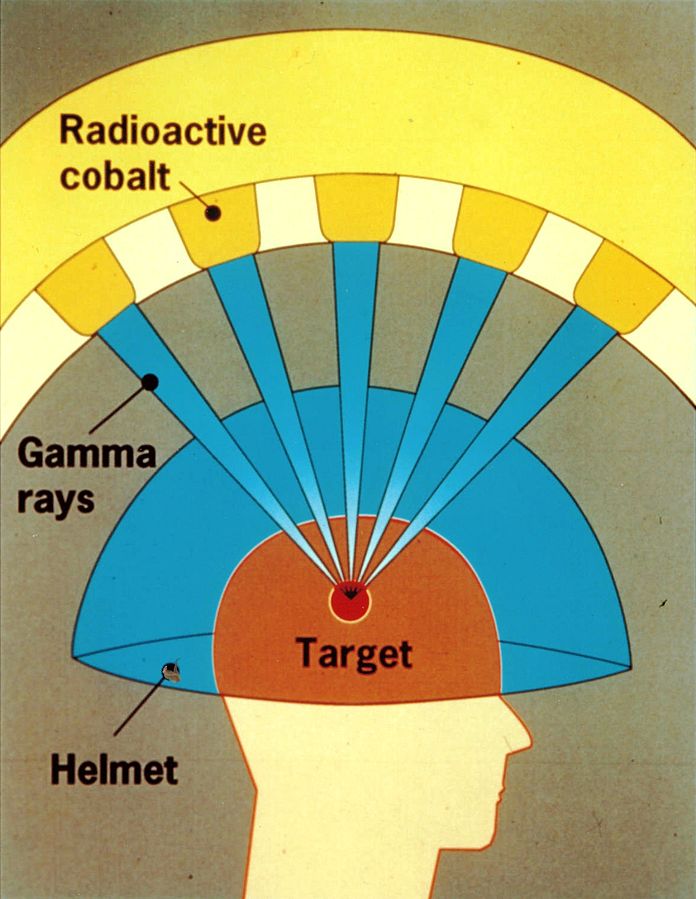
Why Isn’t CyberKnife, Radiosurgery Common Brain Tumor Treatment?
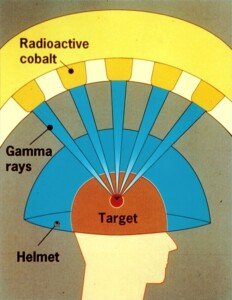
CyberKnife and other kinds of radiosurgery aim a beam of radiation directly to a brain tumor, sparing damage to healthy surrounding tissue.
Yet many people with a brain tumor undergo only manual surgery to remove the cancer. (more…)

Brain Tumor Can Cause Smelling Something Bad that’s Not There

One possible cause of smelling something bad that’s not there is a brain tumor.
The brain tumor causes seizure activity that leads to smelling odors that have no outside source. (more…)

Can Lifting Weights Cause a Winged Scapula?

Lifting weights can cause a number of injuries involving the shoulder and back, and many weightlifters wonder if a winged scapula can be one such injury. (more…)

Can a Winged Scapula Have No Pain Symptoms?

You can have a “winged scapula” and not even know it.
When’s the last time you looked at your upper back in a mirror? A winged scapula can progress and require treatment. (more…)

How to Prepare the DigniCap® Chemo Hair Loss Prevention

Here are the instructions simplified on how to prepare the DigniCap® for the prevention of hair loss during chemotherapy.
Wetting the Hair
• Make sure hair is washed first at home before attending the treatment.
• Thoroughly wet hair; very important.
• Comb wet hair flat.
Cap Size and Fitting
• The silicone cap must be fitted very closely to patient’s scalp, covering all the (wet) hair.
• Do not let air get trapped between the cap and the scalp, as this will interfere with the cooling.
• There are different size caps available: XS, S, M and L.
• Minimize breaks during infusion.
Application of Cooling Cap
• The silicone cap goes on, followed by the neoprene outer cap.
Connect Cap to Cooling Unit
Begin the Scalp Cooling Treatment
• Hospital staff operates the cooling and control unit, not the patient.
• The target temperature is 37-41° F (3-5° C).
Completion
Let hair dry naturally.
In addition to these preparation instructions for the DigniCap® chemo hair loss prevention system, it’s important how you care for your hair between infusions.
• Avoid daily shampooing.
• When you do shampoo, use lukewarm water and gentle shampoo.
• Avoid heat applications—all of them.
• Avoid peroxides, perms, parabens, sodium laurel sulfate, silicones or “anti-frizz” ingredients.
• Don’t brush or comb more than twice a day, ideally once. Use a wide tooth comb.
• Avoid rubberbands and headbands.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: dignicap.com/patients/
How to Prevent Hair Loss from Chemotherapy: the DigniCap
The DigniCap hair preservation method is capable of preventing just about all hair loss from chemotherapy.
In some patients. You don’t know if you’ll be one of the lucky ones. (more…)

Why Do Onions Make You So Hungry?

Have you noticed that soon after eating anything with onions, you’re so hungry you can eat a horse?
And this hunger from onions is relentless, because you keep eating afterwards and the hunger is still deep. (more…)


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}