
Why Diabetics Should Avoid Nutella: Healthy Alternatives

What’s up with all the hype about Nutella being a health food?
This stuff is junk food and no good for diabetics. Don’t let the catchy funky name “Nutella” mislead you. (more…)

Edema from Fat Look Different than Edema from Heart Failure?

Excess body fat causes edema, but so does chronic heart failure.
Here is a comparison in how this swelling looks on the body when it’s caused by either of these two common conditions.
When a person has excess body fat, what makes them big is the enlargement of fat cells.
A person’s legs can be quite big from excess body fat. Sometimes this fat can look edematous: consisting of edema.
When a thin person has edema from chronic heart failure, it’s very obvious. An overweight person, too, can have edema from heart failure.
And then there are overweight people who don’t have heart failure but fear that they do because they think there’s edema in their legs and even belly.
Does edema from fat look different than edema from chronic heart failure?
“Edema from heart failure is a collection of fluid under the skin which is primarily located in dependent (lower) portions of the body, especially the ankles and legs,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths and Tricks: A Physician’s Advice.”
“It results from increased pressure in the veins enhanced by gravity in the presence of impaired ability of the heart to clear blood from these lower bodily veins, and as a result, the fluid components of the blood leak out into surrounding tissues,” explains Dr. Tavel.
“Edema from heart failure is usually manifest as a puffiness in the ankles, which is ‘pitting’ in nature, i.e., light pressure by the fingers leaves small pits in the skin remaining for a short time after the pressure is released.” This is called pitting edema.
Edema from chronic heart failure often appears worse at night.
“Despite a similar appearance, this characteristic usually allows its distinction from ‘puffiness’ resulting from fat under the skin found in obese people,” continues Dr. Tavel.
“This latter type of swelling does not ‘pit’ in response to external pressure, since the pitting [from heart failure] results from fluid that has escaped into the surrounding tissues.
“Moreover, puffiness in the obese may extend to all portions of the body, not just the lower extremities.” Further, it won’t look worse at night.
Pitting from Other Causes
Dr. Tavel explains, “Occasionally, however, obese people — and occasionally those who are not obese — will exhibit swelling that does pit, which may result from buildup of pressure in the veins of the legs after prolonged sitting or standing.
“In this latter instance, however, additional signs of heart failure, such as shortness of breath on exertion or evidence of reduced heart function on various testing means [namely, an echocardiogram], are absent. Neither type of swelling is typically associated with pain.”

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/JAOWFAH
Causes of Baseline High Blood Pressure in a 25-Year-Old

How is it that a person as young as 25 could have a baseline blood pressure that’s high, meaning at least 140 for the top number and over 90 for the bottom number? (more…)

Should People with Stiff Backs and Legs Do Yoga?

Good news for those with stiff backs and legs who are wondering if they could benefit from or even try yoga!
Do not blow off yoga just because your back is as stiff as a plank of wood or because your legs feel like wooden sticks. (more…)
Are Squats, Deadlifts and Lunges Safe During Pregnancy?

An OBGYN was squatting at the gym the day she gave birth to her daughter and explains how to safely perform squats, deadlifts and lunges during pregnancy.
The answer to “Can I do squats, deadlifts and lunges during pregnancy?” is not quite as straightforward as the answer to “Should I avoid smoking during pregnancy?”
“This is a tricky question because there are many factors involved,” begins Mylaine Riobe, MD, founder of Riobe Institute of Integrative Medicine.
Dr. Riobe, who’s board certified in ob/gyn and integrative medicine, is the author of “The Answer to Cancer” and has over 15 years’ experience using integrative techniques to treat diverse patients.
Dr. Riobe continues, “If a woman has already been lifting moderate weights long term prior to her pregnancy, and her pregnancy is uncomplicated in any way, it’s fair to say that she can continue to lift weights under physician supervision.
“Certain precautions must be taken including proper nutrition, hydration and balance. During the first trimester in such a case, there are minimal restrictions.
“At the outset of the second trimester, it’s important to avoid lying flat on the back; this can cause the uterus to block the major veins (the vena cava) and cause poor blood flow.”
So while the squat, deadlift and lunge are definitely in, during the second trimester, the bench press is definitely out!
“It’s important to be standing or inclined, and not flat,” says Dr. Riobe.
“I’m an avid weightlifter and I exercised throughout my pregnancy and was squatting at the gym the day I had my daughter, so it’s very doable, with proper caution.
“If the pregnancy is complicated in any way, it’s imperative to discuss exercise with your physician to see what specific restrictions would apply.”
Detailed Guidelines for the Squat, Deadlift and Lunges While Pregnant: Do Them Safely
As Dr. Riobe explained, if your body was trained in the squat, deadlift and lunges prior to becoming pregnant, and your body is thus used to the demands of this kind of training, then it’s a go – within the context of letting how you feel during the workout dictate whether or not it’s time to take a break or cease for the day.
Even a very trained woman who warms up with a 135 pound squat can suddenly become nauseous; you’d better rack the bar and have a seat, and perhaps call it a gym day.
No matter how trained you are, plenty of hydration and nourishment is crucial. Munch on grapes or a banana between sets, for instance.
For trained as well as novice women, the factor of balance equally applies. Just be careful you’re not moving through the gym in a way that can cause a fall.
Gee, eagerly trotting up the staircase to the free weight area could result in a stumble and hard fall to the steps.
- Watch where you’re walking on the gym floor. Tripping hazards are always present.
- Be careful in the locker room where puddles of water on the floor can cause a slip-and-fall.
An expectant woman is actually more likely to sustain damage to her body simply falling or losing her balance doing some nutty one-legged routine than from keeping both feet on the floor during a barbell or kettlebell squat.

Shutterstock/Serghei Starus
What about exertion?
Go for it, as long as #1) You feel good, and #2) You’re not putting yourself at risk for losing balance such as attempting squats while standing on a BOSU board.
Your primitive ancestors, when pregnant, didn’t have the luxury of driving or Uber to get around.
They had to walk long distances on rough terrain and carry buckets of water, firewood or whatever, sometimes with a toddler strapped to their back!
The human body—including female—was designed for physical exertion. The old school of thought was for pregnant healthy women to “take it easy.”
The new school of thought among ob/gyns is that structured exercise helps lower the risk of pregnancy related complications, gestational diabetes, delivery problems and low birth weight.
Exercise during pregnancy will also help with food cravings and mood swings.
Untrained Women Who Want to Get in Shape While Pregnant
There is nothing inherent in the motions of the squat, deadlift and lunge that increase the risk of miscarriage or other pregnancy related complications.

Shutterstock/Paul Aiken
These multi-joint motions are simple, steady and non-erratic. There is no jumping, impact or sudden changes of direction.
And don’t forget that with the squat, deadlift and stationary lunge, you’re standing in one spot the entire time with both feet on the floor at all times. How safe is THAT?
Basic Safety Guidelines
• Always warm up by doing the exercises you intend to train at.
• Hydrate prior to workout.
• Have quick-acting carbs readily available.
• Before you progress in amount of resistance, make sure you have nailed excellent form.
• Don’t try to set records.
• Never hold your breath during a lift. Exhale on the exertion and inhale on the release.
• Stop if you feel ill or not right.
Deadlift During Pregnancy Safely

Shutterstock/Paul Aiken
• What’s “heavy” is relative. Do five to 10 reps of whatever weight challenges you.
• After the last rep, lower the bar carefully.
• Be a stickler for perfect form!
Squat During Pregnancy Safely
• If the back squat is uncomfortable, try other versions such as holding dumbbells at your shoulders or with straight arms; the Smith machine or the plie squat (shown below).

Plie squat. Freepik.com
• Be a stickler for perfect form!
Lunge During Pregnancy Safely
• This can be done stationary or walking-style.
• Hold dumbbells with straight arms or press them over your head.
• Do not round your back or lurch forward. If you must lean forward, the weight is too heavy.
• You can also hold a weight plate or heavy ball at your chest.
Never let other issues stop you from strength training while expectant. These include feeling “too fat,” “too bloated” or believing you’ll endanger your baby’s health.
If you hydrate and nourish, follow general exercise guidelines for pregnant women, use good form and avoid balance moves — the squat, deadlift and lunge will be among the best things you can do for your baby.

Dr. Riobe has helped thousands of patients overcome difficult illnesses by addressing root causes, not just masking symptoms. The Riobe Method focuses on the prevention of disease, not the prevention of death from disease. She has 20+ years’ experience using integrative techniques to treat diverse patients.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com/drobotclean
Why Aren’t All CIN 1 Cases Treated with LEEP?
![]()
If it’s possible to go from CIN 1 to CIN 3 in 90 days, why aren’t all CIN 1 cases treated with LEEP?
CIN 1 is precancer and has the potential to transform into a full-blown malignancy if left untreated. CIN stands for cervical intraepithelial neoplasm.
The key word here is “potential.” It’s not a guaranteed future malignancy.
Nevertheless, it needs serious attention — but not necessarily aggressive.
In general, Pap smears are recommended for sexually active women on a yearly basis, and women should discuss with their doctors what screening protocol is best for them, based on their personal and medical history.
Sometimes, the Pap smear reveals a degree of abnormal cell growth that’s classified as CIN1.
“CIN1 can resolve in 50 percent of cases, so conservative management in a compliant patient is usually undertaken,” says Mylaine Riobe, MD, founder of Riobe Institute of Integrative Medicine.
Dr. Riobe, who’s board certified in ob/gyn and integrative medicine, is the author of “The Answer to Cancer” and has over 15 years’ experience using integrative techniques to treat diverse patients.
“If the CIN 1 doesn’t resolve after a year, then a more definitive treatment is recommended,” continues Dr. Riobe.
“CIN is usually a slow growing process that takes several years; however, in patients with immune deficiencies such as smokers, those with HIV or other immuno-compromised states, can experience more rapid progression.
“Once CIN 1 is diagnosed, Pap smears are done every three months rather than annually.
“This increases the surveillance so that rapid progression can be detected and successfully treated.”
Why not LEEP for All CIN 1 Cases?
Dr. Riobe explains, “LEEP is an invasive surgical procedure that can lead to a condition called cervical incompetence in a small number of patients (one in 1,000).
“Cervical incompetence leads to premature vaginal deliveries often in the second trimester of pregnancy before the baby is viable.
“It’s a condition that is difficult to prevent, so it’s best to avoid a LEEP if it’s not necessary. LEEP is usually recommended for CIN 2-3 and has a 96 percent success rate and a 4 percent rate of recurrence if all the affected tissue is successfully removed.”
LEEP stands for loop electrosurgical excision procedure.
Dr. Riobe has helped thousands of patients overcome difficult illnesses by addressing root causes, not just masking symptoms. The Riobe Method focuses on the prevention of disease, not the prevention of death from disease. She has 20+ years’ experience using integrative techniques to treat diverse patients.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Shutterstock/Pixel-Shot

Could a D & C Detect Ovarian Cancer?
A “D & C” stands for dilation and curettage and is very useful at detecting uterine cancer, but some women are wondering if ovarian cancer as well can be detected by this procedure. (more…)

Can a Virgin Get CIN 1 (Cervical Dysplasia)?

If you’re a virgin and have CIN 1, and your doctor won’t believe you’re a virgin, it’s highly recommended that you find yourself a new doctor.
That’s because virgins CAN get cervical intraepithelial neoplasia, which is precancer of the cervix. (more…)

The Link Between “Skinny Fat” and Breast Cancer
It’s now been shown that being “skinny fat” puts a woman at a higher risk of invasive breast cancer.
This in part explains why “thin” women can get just as sick as full figured women. (more…)

Ovarian Cancer Ascites vs. Belly Fat: Telling the Difference

Belly fat may grow so quickly and stick out so much that you fear it’s actually ascites from ovarian cancer, but there are ways to tell the difference.
“The diagnosis of ovarian cancer is extremely difficult and symptoms can remain hidden for months or years because they tend to be vague,” begins Mylaine Riobe, MD, founder of Riobe Institute of Integrative Medicine. Dr. Riobe, board certified in OB/GYN and integrative medicine, is the author of “The Answer to Cancer.”
Dr. Riobe continues, “Because the ovaries are attached to the wall of the abdomen by a ligament and otherwise are free-floating in the abdomen, masses can grow to enormous sizes before being detected on examination.
“It’s important to have a low threshold to evaluate vague symptoms such as onset of persistent bloating [which could be caused by ascites], increase in the girth of the abdomen [again, ascites], pelvic pain, abnormal vaginal bleeding, nausea and malaise.
“Ascites is a late finding in ovarian cancer and is fluid in the pelvis and abdomen.”
There are ways that doctors can distinguish between ascites from ovarian cancer and abdominal distension from belly fat.
However, while you wait for your doctor appointment, there are things you can check for that would point far more to belly fat than ascites.
But keep in mind that you may have BOTH increasing belly fat and ascites.
Ascites will make the abdomen get bigger and increase in circumference without a proportional increase in fat elsewhere.

Massive ascites from ovarian cancer, which had been progressing for six months without treatment. Note absence of “rolls of fat” despite belly size.

Same patient. During that time this 70-year-old patient had weight LOSS. Note the dramatic disparity between size of abdomen and size of limbs. Courtesy: Tom Baker Cancer Centre, Calgary, Canada
However, the phenomenon of an increasing abdominal girth in the absence of increasing size elsewhere in the body occurs to many people who do not have ascites.
We’ve all seen people with scrawny or non-overweight arms and legs who have ever-growing bellies.
This phenomenon is particularly prevalent in people over 50 who have never strength trained and who lead sedentary lives.
Belly Fat and Ascites: Unique Features of Each
• If enough increasing amount of fat is getting stored in your abdomen, you should also be able to see an increasing amount of fat at your waist and a little behind it, towards the back — and if there’s enough of it, you’ll be able to grab it like bread dough.
• Nobody gains only a lot of fat in the belly while their sides and back remain lean.
Look at the sides and backs of women with fatty potbellies. There are clear signs of excess fat deposits.
• As the belly grows from fat storage, you will be able to pinch an increasing amount of blubber at your sides and going towards the back.
• A blubbery stomach with no ascites will have at least one “roll.” If there’s even only one, you will see this when viewing the profile or three-quarter view — as in the image below.

Shutterstock/L Julia
The stomach will cave in at the middle, then puff back out. In an abdomen free of much excess fat but full with excess fluid, this cave-in area will be absent — as in the previous image.
• If you eliminate junk food and practice portion control, and increase your exercise enough to create a marked daily caloric deficit, you’ll lose several pounds of fat quickly, causing a visible reduction in your abdominal girth when viewed profile.
• If you have ascites, you cannot diet or exercise it down.
• A visible gain in belly size over just one week does not necessarily mean ascites if you’ve been eating way more than usual.
And if you’re as hungry as you’ve always been, and especially hungrier than ever, chances are pretty high that you don’t have excess abdominal fluid — because this classically causes appetite LOSS.
• In yo-yo dieters in which the cycle of weight gain and loss repeats itself, the appearance of the abdomen will also fluctuate.
However, ascites from ovarian cancer will not come and go.
• Often, ascites is accompanied by a feeling of persistent bloating.
• Ascites may also cause difficulty breathing because the excess fluid interferes with diaphragm function.

Patient is 25 with ovarian cancer ascites. Note exceptionally smooth and taut appearance of skin; no “blubbery” features or rolls of fat. International Journal of Case Reports and Images.
• In ovarian cancer, a thin woman’s stomach may just keep expanding while the rest of her remains thin.
Her belly won’t have that classic blubbery look of overweight.
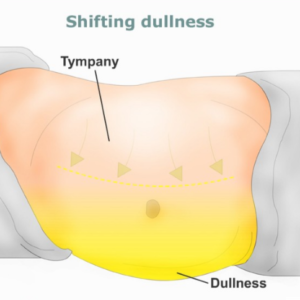
Finally, if you’re lying on your side and notice a shift of your belly downward, this is a sign of ascites…as depicted below. The yellow area would be the ascites.
Mild Ascites vs. Mild Abdominal Fat
“It’s not really possible to distinguish mild ascites from belly fat,” says Dr. Riobe, referring to the layperson staring at their abdomen in the mirror.
“A CT scan or ultrasound would quickly distinguish between the two.
“I would not recommend that anyone try to distinguish the two without medical assistance, as time is of the essence in the case of ovarian cancer.
“The sooner it’s diagnosed, the better the outcome.”
How Doctors Test for Ascites from Ovarian Cancer
“When the abdomen is ‘percussed’ by the physician (vaguely beaten like a drum with one finger over the other), the abdomen should sound hollow,” says Dr. Riobe.
“If it doesn’t then that may be an indication of a mass or fluid. You can also tilt the patient and percuss to see if there is fluid in the abdomen.
“This is not a precise examination by any means but can give some information during a workup.
“A pelvic exam, radiological study such as CT or ultrasound and blood work called CA-125 can assist in the diagnosis.
“A definitive diagnosis is obtained by removal of a visible mass and examination by a pathologist to determine the tissue type and diagnosis.”
The presence of new-onset symptoms such as gas, constipation, feeling full after small meals, suppressed appetite, fatigue and pelvic or lower abdominal cramps – plus an expanding abdomen despite no increase in food intake – and especially a reduction in food intake – is highly suspect for ovarian cancer.
Conditions other than cancer can cause these symptoms, though if ascites is confirmed, you have a serious condition nevertheless – even if it’s not ovarian cancer.
This is because no benign condition causes ascites. In fact, most cases of ascites are caused by liver problems.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}