

Pooping After Every Meal: Causes and Solutions

Sick of having to make a poop after every meal and wondering what’s causing this?
There are actually multiple possible causes for having to make a bowel movement shortly after just about every meal.
“One of the things to worry about is insufficient enzyme production by the pancreas,” says Matilda N. Hagan, MD, an inflammatory bowel disease specialist at The Center for Inflammatory Bowel and Colorectal Diseases, a part of The Melissa L. Posner Institute for Digestive Health and Liver Disease at Mercy Medical Center in Baltimore.
“This can cause mal-digestion and malabsorption, leading to pooping after meals,” says Dr. Hagan.
A condition called exocrine pancreatic insufficiency is when the pancreas doesn’t produce enough enzymes.
Causes of EPI
• Chronic pancreatitis (causes include heavy drinking, smoking, high triglycerides, lupus, Sjogren’s syndrome, type 1 diabetes, or blockages in the passageways from stones or tumors)
• Recent surgery on the pancreas, intestines or stomach
More Causes of Pooping After Most Meals
“Some people can have bile acid diarrhea which is worse if the gallbladder has been removed,” says Dr. Hagan.
“In this case people may commonly poop after every meal especially if it is a greasy or fatty meal.
“For some, this may be how their system functions, and when it is their normal state, there usually is no abdominal pain or bloat related to this.”
Solutions to Having a Bowel Movement after Every Meal
Dr. Hagan says, “Depending on the cause, there are specific strategies from changes in diet to medications that should be discussed with a health care provider.”
A benign condition called microscopic colitis may make it seem that every meal sends you straight to the toilet.
In the literal sense, this is not true, but if the diarrhea that’s associated with this condition is frequent enough, it may seem that you are having a bowel movement (albeit diarrhea) after every meal.
 Dr. Hagan is dedicated to collaborating with IBD specialists to discuss and explore advanced treatment options for the most complex inflammatory bowel disease cases.
Dr. Hagan is dedicated to collaborating with IBD specialists to discuss and explore advanced treatment options for the most complex inflammatory bowel disease cases.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Frepik/gpointstudio

“Tarry Black” Stools Defined by a GI Doctor

“Tarry black” stools defined by a doctor, NOT Yahoo Answers!
Once and for All, Here Is What Tarry Black Stools Look Like
“In the simplest sense, the stool has the look and consistency of tar used to pave the road,” says Matilda N. Hagan, MD, an inflammatory bowel disease specialist at The Center for Inflammatory Bowel and Colorectal Diseases, a part of The Melissa L. Posner Institute for Digestive Health and Liver Disease at Mercy Medical Center in Baltimore.
Have you ever seen small chunks or clumps of moist, solid tar on a freshly paved road? It doesn’t go from a hot liquid to solid dry concrete in an instant.
Remnants of tar do make their way off the side of a road while it’s being paved.
And if you’ve ever seen these clumps while they’re still somewhat wet, but not hardened and dried, you can almost imagine that stools might look something like this—if mixed with old blood from the upper colon.
Dr. Hagan explains, “This term [tarry stools] describes blood in the stool, especially blood that has been processed or digested from the upper intestinal tract.
“If you see black stool, you should consult a health care provider.”
Imagine taking a quarter cup of hot tar and mixing it with typical formed stools.
What would you see? This is more like what tarry black stools would look like, versus tossing in clumps of moist, partially solidified road tar into an empty toilet and pretending that this matter is a collection of poops.

“Tarry stools”
But don’t get caught up with the exact definition of “tarry.”
Black smeary stuff mixed with your BMs is an alarming sign — though this doesn’t always mean colon cancer.
A tarry look to your stools can mean an ulcer or side effects from medications.
Dr. Hagan is dedicated to collaborating with IBD specialists to discuss and explore advanced treatment options for the most complex inflammatory bowel disease cases.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Ronald Plett

What Diarrhea Alternating with Constipation Really Means

Confused over what “diarrhea alternating with constipation” actually means?
The commonly used phrase, diarrhea alternating with constipation, is sometimes seen in symptom lists for colon cancer and IBS, even ovarian cancer.
And it’s ambiguous.
Alternating Diarrhea and Constipation with IBS
“Generally speaking, ‘diarrhea alternating with constipation’ is specific to ‘mixed type irritable bowel syndrome,’” begins Matilda N. Hagan, MD, an inflammatory bowel disease specialist at The Center for Inflammatory Bowel and Colorectal Diseases, part of The Melissa L. Posner Institute for Digestive Health and Liver Disease at Mercy Medical Center in Baltimore.
“This means a person has changes in their bowel habits such that at times they have diarrhea (well-known to be change in consistency of stool from formed to loose or liquid) or constipation where there is a decrease in frequency of bowel movement and/or passage of hard pellet-like stool.
“For some they may have normal formed stool in between or go from one extreme to the other.
“As far as timing, skipping three or more days without a bowel movement counts as constipation, especially if it is associated with abdominal discomfort or bloat.”
Alternating Diarrhea and Constipation with Colon Cancer
You may have read that colon (or ovarian) cancer may cause “diarrhea alternating with constipation.”
The aafp.org site states for colon cancer: “Constipation may be constant or may alternate with diarrhea.”
It’s that word “alternate” or “alternating” that throws things off.
The aafp.org site states that in colon cancer, the “alternating constipation and diarrhea signify leakage of liquid stool” that’s “around the lower level of a tumor.”
The cancer is “partially obstructing the bowel.”
What else can alternating diarrhea and constipation mean?
As Dr. Hagan explains, relative to IBS, it’s a time period of diarrhea, followed by a time period of constipation, and constipation is defined as three-plus days without a bowel movement and/or voiding hard, pellet stools.
Constipation can also mean straining hard to void hard stools, not necessarily pellet shaped.
They can be larger chunks — but hard, necessitating a lot of straining and discomfort while you’re on the toilet seat.
You may even be having normal frequency of BMs, but nearly every time, they are hard and require heavy straining.
What if in between these episodes, you have diarrhea?
This would fall under the category of “alternating.” The in-between episodes themselves can vary.
For instance, Monday, Tuesday and Wednesday you have BMs—all hard and requiring straining.
But Thursday you have diarrhea. Friday you strain and void hard poops.
Saturday, diarrhea. Sunday, diarrhea. Monday, a few hard, straining bowel movements. Wednesday, diarrhea.
You get the picture. Any given day is either all diarrhea or all constipation.
Another scenario is that on a given day, you have both diarrhea and constipation. The day after may be all diarrhea — or all constipation.
Or maybe in between normal voiding days (formed non-hard stools), you have days of both constipation and diarrhea.
There are benign causes like IBS and food intake, but potential (less likely) serious causes like colon and ovarian cancer, and Crohn’s disease.
In short, the concept of diarrhea alternating with constipation comes with multiple permutations.
No particular permutation points to colon or ovarian cancer!
Dr. Hagan says, “If the symptoms are present for three months or longer,” you should “consider discussing with a health care professional.”
However, if the symptoms come with other issues such as unexplained weight loss, stomach or pelvic pain, back or leg pain, poor appetite or new-onset fatigue, don’t wait longer than two weeks to make a medical appointment.
If you see blood in your stools, make the soonest appointment possible. This is never normal.
Dr. Hagan is dedicated to collaborating with IBD specialists to discuss and explore advanced treatment options for the most complex inflammatory bowel disease cases.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Africa Studio
Source: aafp.org/afp/2000/0315/p1759.html#sec-7
Gray Stools: Causes & Should You Worry?

Yes, you should worry if your stools are gray.
Gray stools are concerning. Sometimes when doctors talk about grey stools, they use the terms “clay colored” or “pale.”
However, “clay” can bring up images of bowel movements that are the color of the standard clay pot that people plant flowers in: a dull or salmon-like orange.
But the “gray” here is an actual greyish hue, like what would result if you mixed white paint with black.
Causes of Gray Stools
“A person’s usual stools in terms of color, shape and consistency are based on their diet,” begins Franjo Vladic, MD, a board certified gastroenterologist with Center for Digestive Health and Endoscopy Center in Ohio.
“However, if a person’s stools are clay colored or pale, health care providers will be concerned about the patient’s biliary system,” continues Dr. Vladic.
“Clay” refers to the greyish type of clay-like substance that’s found in the ground, rather than the common dull orange color of clay pots for plants.
Dr. Vladic continues, “This could be a sign of bile duct obstruction (gallstones, pancreatitis, inflammation of the liver or pancreatic cancer).
“Clay colored stools indicate the biliary system is not draining properly because of a blockage.
“If the system drains properly, stools will either present as shades of green to brown.” They will not be grey.
Pancreatic Cancer
The American Cancer Society estimates that in 2016, about 53,070 people in the U.S. (27,670 men, 25,400 women) will be diagnosed with pancreatic cancer.
Risk factors that can be changed: tobacco use; obesity as well as being overweight primarily in the midsection though not very overweight elsewhere; exposure to dry cleaning and metal working chemicals; lack of exercise (according to some studies but not all).
Uncontrollable risk factors: age, being black (a mild risk that’s not understood), family history, genetic syndromes, diabetes (type II mainly), chronic pancreatitis, liver cirrhosis, pylori stomach infection.
Other Causes of Bile Flow Obstruction
Primary sclerosing cholangitis is a chronic liver disease that causes inflammation and scarring of the bile ducts, which can eventually lead to their obstruction.
Biliary stricture is a narrowing of the bile ducts, often due to injury, surgery or chronic inflammation.
Biliary atresia is a congenital condition in which the bile ducts are absent or malformed.
Liver cirrhosis and other forms of liver disease can cause scarring of the liver tissue, which can compress and obstruct the bile ducts.
“If the stools are not pale or clay colored, the color is affected by the patient’s diet,” says Dr. Vladic.
The exception is reddish or black stools from actual blood.
Don’t be afraid to check your stool color every now and then; grey means you must see a doctor.

Dr. Vladic’s special interests include acid reflux, colitis, colon cancer, GERD, heartburn, IBS, liver disease, obesity, pancreatitis and peptic ulcer, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: cancer.org/cancer/pancreaticcancer/detailedguide/pancreatic-cancer-key-statistics

Can Accutane and Celebrex Cause Blood in Your Stools?

Wouldn’t it be a relief to know that the blood in your poops is from Accutane rather than from an intestinal ulcer, or worse yet, cancer of the colon?
Seeing blood in the toilet after having a bowel movement is just plain scary.
It can have a number of causes including colon cancer. But what about the medication Accutane?
“Yes, Accutane has the potential to present as blood in stools,” says Franjo Vladic, MD, a board certified gastroenterologist with Center for Digestive Health and Endoscopy Center in Ohio.
Accutane is a medication that’s prescribed for acne. Make sure that you read the insertion that comes with this prescription drug to get acquainted with possible side effects.
How often do you look at your bowel movements?
It is so important to know what is a normal appearance and color of your bowel movements.
A normal color ranges from tan to very dark brown. A green tinge is normal if you’ve been eating a lot of greens.
You should periodically check the toilet bowl; take a good look at your poops before flushing.
Make sure that the toilet bowl is always clean so that viewing is not affected. Good lighting will also help in the inspection.
Dr. Vladic explains, “Accutane (isotretinoin) has the potential side effect of aggravating or triggering inflammatory bowel disease in susceptible individuals.
“How it causes these colitis-type symptoms is not clear, but Accutane can cause ulceration and inflammation in the gut mucosa (lining of the gut).”
What about Celebrex causing blood in your BMs?
You’ve certainly seen all the commercials for Celebrex, a pain reliever.
“Celebrex is a medication that can cause blood in stools, similar to aspirins or nonsteroidal anti-inflammatory medications by increasing the risk of ulcerations in the GI tract,” says Dr. Vladic.
“This medication affects the GI tract directly.”
If you’ve noticed blood in your bowel movements and have recently started on Celebrex or Accutane, or any other medication that can potentially cause this — you should alert this to your prescribing physician.
After all, the presence of these drugs in your system wouldn’t guarantee that they’re the cause of bleeding in your colon; you should still get checked out.
Dr. Vladic’s special interests include acid reflux, colitis, colon cancer, GERD, heartburn, IBS, liver disease, obesity, pancreatitis and peptic ulcer, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Nomad_Soul

Flat Ribbon Stool Causes other than Colon Cancer

Are your stools coming out like flat ribbons and scaring the daylights out of you?
If so, you’ve no doubt read or heard that colon cancer can cause BMs to come out in the shape of flat ribbons.
If this happens what should you do?
When someone notices ribbon stools, “the medical provider is concerned about the possibility of colon obstruction or IBS,” says Franjo Vladic, MD, a board certified gastroenterologist with Center for Digestive Health and Endoscopy Center in Ohio.
Dr. Vladic continues, “If there is an obstruction, it’s because there is something in the lumen [lining] of the colon causing it to be thin (i.e., a large colon polyp, narrowing from stricture, or mass).”
Yes, a benign polyp can cause flat ribbon stools by partially blocking the anal exit that BMs would go through, causing the feces to take on this peculiar formation.
A polyp has a good chance of evolving into colon cancer if not removed, so that’s why during a colonoscopy, any polyps that are discovered are removed on the spot — as shown below in the illustration.
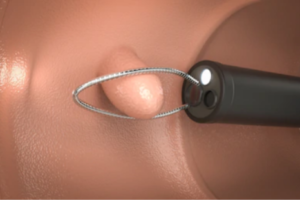
Schematic of polyp removal inside the colon. Shutterstock/Phonlamai Photo
A “mass” can be cancer in the colon—which would be discovered in a colonoscopy, removed and sent to a pathology lab for a confirmation biopsy.
“For IBS, stools can be flat, but providers are unaware as to what causes the stool to present this way,” says Dr. Vladic.
Bottom line: If you notice your stools are in the shape of flat ribbons, see a doctor. Do not make assumptions.
Other Symptoms of Colon Cancer
(No particular order)
Abdominal pain
Unexplained diarrhea
Unexplained constipation
Blood in your stools. This can appear as red clots, maroon clots or like a black tarry or gooey substance.
Unexplained weight loss
Feeling you have to have a bowel movement even though you just had one.
Fatigue or weakness for no reason
Cologuard for Colon Cancer Screening

A test called Cologuard can be taken at home if you’re worried about colon cancer or have flat ribbon stools.
It works as follows: A sample of your bowel movement is sent out for analysis with state-of-the-art DNA technology that will detect abnormal cells that are suspicious for colon cancer.
Your doctor can then advise you on undergoing a colonoscopy.
Another Suspicious Symptom
When constipation alternates with diarrhea, you should inform your doctor. Here is exactly what “constipation alternating with diarrhea” means.
Dr. Vladic’s special interests include acid reflux, colitis, colon cancer, GERD, heartburn, IBS, liver disease, obesity, pancreatitis and peptic ulcer, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Colon Cancer Related Constipation vs. IBS Stools

Here’s a comparison between colon cancer related constipation & IBS.
“Constipation as a symptom itself can be caused by colon cancer or irritable bowel syndrome (IBS) with predominant constipation,” says Franjo Vladic, MD, a board certified gastroenterologist with Center for Digestive Health and Endoscopy Center in Ohio.
Can you tell the difference between constipation from IBS and that from colon cancer?
Dr. Vladic says, “IBS with predominant constipation is a benign condition, meaning that the patient does not present with any alarm symptoms, such as unintentional weight loss, blood in stools, abdominal distention, nausea or vomiting.
“If a patient presents with any of these alarm symptoms, coupled with constipation, their provider should consider an organic etiology being the cause of the constipation.
“Without any alarm symptoms, the constipation is likely from IBS or another benign condition that should not cause any potential concern.”
Does colon cancer related constipation look different than IBS constipation?
When colon cancer causes constipation, there is nothing compositionally different about the stools vs. when the constipation has a benign cause such as irritable bowel syndrome.
The constipation from colon cancer is caused by an obstruction in the colon, which holds the stools back, preventing an easy void, or delaying a void (the tumor can shift out of the way, allowing backed-up stools to finally void).
IBS does not involve any abnormal composition of stool matter, either.
Thus, the appearance of the stools, from colon cancer related constipation, would be the same as that from IBS, when the patient views the BMs in the toilet bowl.
The big variable is the absence—or presence—of those other alarming symptoms.
But here’s something to consider:
It’s entirely possible to have both IBS and colon cancer.
If you’re worried, consider a home stool test called Cologuard, which uses state-of-the-art DNA technology to detect abnormal cells in feces.
The Cologuard kit
Dr. Vladic’s special interests include acid reflux, colitis, colon cancer, GERD, heartburn, IBS, liver disease, obesity, pancreatitis and peptic ulcer, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Aaron Amat

Colon Cancer Change in Bowel Habits vs. IBS

Is it possible to tell the difference between colon cancer’s “change in bowel habits” and the change in IBS?
“Both colon cancer and IBS can have constipation and abdominal cramps,” begins Franjo Vladic, MD, a board certified gastroenterologist with Center for Digestive Health and Endoscopy Center in Ohio.
So there you are, suffering constipation and stomach cramps, a pairing of symptoms that is new to you.
Making matters more unsettling is that you’re over 50 — when the risk for colon cancer goes up (though younger adults can get this disease — but that’s much less common).
Is there a difference, though, between this change in bowel habits caused by colon cancer and that which is brought on by irritable bowel syndrome?
Dr. Vladic says that “the features that distinguish between the two is if the patient demonstrates alarm symptoms such as unintentional weight loss, blood in stools, abdominal distention [bloating], nausea or vomiting.
“If those symptoms are present, it can cause more concern and discussion of colon cancer rather than if those symptoms are not there.”
Unexplained fatigue and loss of appetite are two more potential symptoms that can be from colon cancer.
Colon cancer is diagnosed via a biopsy analysis of a suspicious growth that’s found inside the large colon during a colonoscopy. It’s never diagnosed based on symptoms; only suspected.
IBS is diagnosed only when all other conditions are excluded, such as inflammatory bowel disease and side effects of medications.
Irritable bowel syndrome is a diagnosis of exclusion, so be leery of this diagnosis if you have not undergone every possible test to explain your change in bowel habits — especially if you haven’t had a colonoscopy!
An at-home method for colon cancer screening (not diagnosis) can be performed called Cologuard.

The patient sends a stool sample off for analysis, and abnormal cells will be detected with advanced DNA technology.
A follow-up colonoscopy is then recommended.
Dr. Vladic’s special interests include acid reflux, colitis, colon cancer, GERD, heartburn, IBS, liver disease, obesity, pancreatitis and peptic ulcer, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Why Your Hair Smells SO Good!

If you find yourself occasionally smelling your hair, taking big sniffs…there is nothing wrong with you.
This is actually no different than occasionally looking in the mirror and admiring the appearance of your hair.
And how often have you looked at your manicured nails with admiration? Or your painted lips or perfectly shaped eyebrows?
The sense of smell can be very powerful, just as the sense of sight and sound can be.
If something smells good, we will sniff it, whether it is a cinnamon stick, pages of a new magazine, the interior of a new car, a fresh bouquet of flowers, the body lotion from a tube that you rub into your skin after a shower, the shampoo you wash your hair with — and of course — your hair.
Sometimes, a woman can’t help but be aware of her hair’s natural scent, especially when she is lying in bed and her hair is positioned closer to her nose due to the way it lies on the pillow.
Let’s face it, hair often just smells really good. This is why a man will often sniff his wife’s or girlfriend’s hair.
And it goes both ways: A man’s hair can have a naturally glorious scent.
What gives hair its natural smell?

Freepik.com/cookie_studio
It’s not shampoos or other agents that you put into it, though these external agents will mix in with your hair’s natural scent.
But as days go on following your last shampoo, the scent of these agents disintegrates, and what your nose is detecting is the scent of the natural oils in your hair.
These oils come from the sebaceous glands in your scalp, says Dr. Robert Dorin, DO, NYC-based hair care expert and restoration specialist.
Sebaceous glands are connected to hair follicles.
“Natural surface bacteria and perspiration” also contribute to the scent of your hair, adds Dr. Dorin.
The oil from sebaceous glands is called sebum.
Sebum
This oily substance lubricates and protects the skin and hair.
By coating the skin’s surface, sebum helps maintain moisture, prevent dehydration and create a barrier against external pollutants and microorganisms.
In the scalp, sebum keeps the hair and scalp hydrated, reducing dryness and brittleness.
The oil of sebum makes its way onto hair shafts, coating them, and also onto your scalp, creating the sweet smell of your hair that you love — or that the man in your life really likes.
The sebum-coating on your hair shafts gets further distributed every time you comb or brush your hair.
So go ahead, don’t be shy about taking a good whiff! The scent of your hair is as unique as your fingerprints.
 Dr. Dorin of True & Dorin provides creative hair loss solutions, including advanced hair transplant techniques and the latest in regrowth technology, to ensure that his clients achieve their desired results.
Dr. Dorin of True & Dorin provides creative hair loss solutions, including advanced hair transplant techniques and the latest in regrowth technology, to ensure that his clients achieve their desired results.
Lorra Garrick has been covering medical, fitness and cyber security topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She is also a former ACE certified personal trainer.
.
Top image: ©Lorra Garrick

Why Your Elderly Mother Is Delirious After Surgery

Are you shocked over how delirious your elderly mother (or father) is after surgery—such as a hip replacement, knee replacement or coronary bypass?
It’s called postoperative delirium, and about half of elderly patients experience this—and it’s linked to the general anesthesia.
My mother at age 88 underwent a hip replacement, and the delirium after the surgery was significant.
You’ll know it when you observe it; it’s not subtle.
For instance, while in the hospital bed, she thought she was at home and that a nearby table was her kitchen desk.
Why an Elderly Patient Develops Postoperative Delirium
A news release came out in August 2015 by the Department of Geriatrics and Gerontology at the Rowan University School of Osteopathic Medicine.
The researchers tested Sevoflurane and Isoflurane, anesthetics that are inhaled during surgery, on animal models. Sevoflurane disrupted the blood-brain barrier, while Isoflurane didn’t.
The study’s lead author, Nimish K. Acharya, PhD, explains in the report that when the blood-brain barrier is disrupted, “various plasma components gain access into the brain” and bind to some neurons, possibly disrupting “normal neuronal activity.”
Dr. Acharya adds that this may “cause the onset of symptoms that define postoperative delirium.”
When I asked nurses and doctors why my elderly mother was so delirious, their standard reply was, “It’s the anesthesia.”
I thought this was just one of those quick, ambiguous responses to a hovering family member, but there was definitely some truth behind this response.
So why are patients who suffer from delirium right after surgery elderly rather than 30-something?
The study’s older animals showed a big increase in the “density and extent of vascular leak” in their cerebral cortexes from the Sevoflurane, says the report.
Robert Nagele, PhD, the study’s corresponding author, explains that a less potent anesthetic for elderly patients should cause less disruption to the blood-brain barrier.
If your elderly mother or other relative is still delirious days after their surgery, don’t panic.
My mother fully recovered from her cognitive impairment, though this didn’t happen overnight. It tapered off. Each patient is different.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}