
How Many People Have Sleep Apnea? It’s Often Misdiagnosed
![]()
Many people have sleep apnea and have no idea they have this dangerous condition, and contrary to myth, thin people CAN have obstructive sleep apnea.
Obstructive sleep apnea is quite prevalent – and not just because so many people are obese.
It’s one of the most under-diagnosed and misdiagnosed medical conditions.
It’s years before many patients are finally diagnosed.
OSA can cause life-threatening complications if not treated.
It does not affect only older overweight men who snore. Younger people including women of normal body weight can be affected.
Why is OSA dangerous?
“Sleep apnea causes high blood pressure — plain and simple, and we know high blood pressure can lead to cardiovascular disease,” says Daniel Rifkin, MD, a sleep medicine expert at the Sleep Medicine Centers of Western New York.
“However, sleep apnea alone, and independent of high blood pressure, is associated with cardiovascular disease.”
Just how many men and women have sleep apnea?
The New England Journal of Medicine says that nine percent of middle age women and 24 percent of middle age men have sleep apnea.
While more conservative estimates say that two to four percent of middle age men and one to two percent of middle age women are affected by sleep apnea, this does NOT account for the vast demographic that remains undiagnosed.
Fact is, most people with sleep apnea, including in societies with the most advanced medicine, are walking around without a diagnosis.
Or, they’re walking around with the wrong diagnosis.
Number of Americans with OSA
The estimation is about 22 million, with 80 percent being at the moderate to severe level. This means over 15 disordered-breathing events per hour of sleep.
One reason obesity is associated with obstructive sleep apnea is because obesity exacerbates daytime symptoms, making patients miserable.

Fj.toloza992, CC BY-SA
Those with troubling daytime symptoms are more likely than thin patients with milder daytime symptoms to seek medical attention.
Hence, obese sufferers may be getting faster and more numerous diagnoses.
Obesity also can also crowd out the upper airway during sleep when it’s most relaxed.
However, craniofacial structure and natural throat anatomy are the driving forces behind OSA.
Shutterstock/iLoveCoffeeDesign
If a skinny person has a large uvula (the “punching bag” that hangs in the back of your throat) in combination with a narrow airway, this is the perfect storm for obstructions during sleep.
Other contributing elements include a large tongue base and surplus pharyngeal tissue.
If this person becomes fat, then the tissue around these structures becomes plumper, increasing the degree and frequency of obstructions.
Many people with undiagnosed OSA are wrongly diagnosed with the following:
• Age related fatigue
• Stress
• Exhaustion from a hectic lifestyle
• Side effects from weight gain
• Chronic fatigue syndrome
• Fibromyalgia
• ADHD
• Depression
• Chronic sinusitis
• Poor nutrition
Not all people with sleep apnea snore, and not all snorers have sleep apnea.
Symptoms of Sleep Apnea
• Morning headaches that quickly dissapate once up and about
• Excessive urine production overnight
• Gasping or snorting during sleep
• Family members witnessing episodes of stopped breathing
• Difficulty concentrating or irritability
• Easily falling asleep while driving, reading or watching TV
• Jaw soreness or dry mouth when waking
 Dr. Rifkin is board certified in both neurology and sleep medicine. He also treats insomnia, RLS and narcolepsy.
Dr. Rifkin is board certified in both neurology and sleep medicine. He also treats insomnia, RLS and narcolepsy.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rawpixel.com
nejm.org/doi/full/10.1056/NEJMoa1306766#t=article
academic.oup.com/bmb/article/72/1/49/272854
sleepapnea.org/learn/sleep-apnea-information-clinicians/
Morning Headache: Brain Tumor or Sleep Apnea?

Waking up with morning headaches can mean a brain tumor or sleep apnea.
This is because when headaches are caused by these two conditions, they typically are present as the patient wakes up for the day.
A person may wake with a headache caused by more benign conditions, but this article compares the brain tumor headache to the sleep apnea headache.

Twitching Middle Finger Explained by Doctor; When to SEE Doctor

If that twitching middle finger is beginning to worry you sick because you googled it and a bunch of ALS sites popped up, here are answers from a doctor who is double board certified: neurology and sleep medicine.

Can You Be Too Old to Benefit from a CPAP Machine?

Even though old age brings with it problems, this does not mean you’re too old to benefit from CPAP therapy if newly diagnosed with sleep apnea. (more…)
What the Typical Person with Sleep Apnea Looks Like
Think the typical person with sleep apnea looks like a beer gutted middle age man with a short fat neck?
Think again!
There is NO typical appearance of a person with obstructive sleep apnea, and here is why:
“Most people think of OSA as associated with obesity, but it’s now understood that it is not just obesity, but actually the anatomical structures of the upper airway that can cause obstructive sleep apnea.” explains Dr. C. Phillip Amoils, MD, a board certified otolaryngologist with SC-ENT Ear, Nose & Throat Specialists in CA.
Once you know the actual cause of obstructive sleep apnea, you’ll never again stereotype patients as being fat people with no necks.
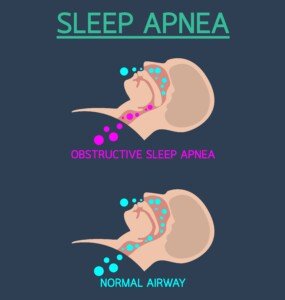
Here’s what happens in obstructive sleep apnea.
Now you may be thinking, “Well gee, obesity causes that to happen.” But what you see in the illustration can occur to thin people, including young women and children.
It has to do with the anatomy we’re born with.
- This could be plus-size tonsils or a large uvula.
- It could be surplus throat tissue – which has nothing to do with obesity.
- It could be a tongue with a big base in combination with a small jaw.
- Or it could be structures that are just prone to excess laxity during sleep.
It can also be acquired via poor lifestyle choices. Smoking causes inflammation of the upper airway tissue. This can lead to obstruction during sleep.
Drinking liquor shortly before bedtime can cause upper airway structures to become way too relaxed, collapsing them — which compromises airflow down the throat.

“I could have sleep apnea.” Shutterstock/Kamira
“I could have sleep apnea.” Shutterstock/ShotPrime Studio

“I could have sleep apnea.” Freepik.com
Obesity is a major risk factor, not the ONLY risk factor.
Of course, obesity adds fat to the throat’s tissue, plumping it up and thereby making the airway smaller during sleep.
In cases of mild sleep apnea, weight loss can eliminate the problem for some patients.
But because obstructive sleep apnea is founded upon structural or anatomical issues, weight loss is not a cure for moderate and especially severe OSA.

Dr. Amoils is considered among the best surgeons worldwide for sinus surgery and OSA, having helped thousands of patients for 30+ years. He also demonstrates to physicians the protocols he’s developed for mouth breathing, nasal congestion, obstructive sleep apnea and snoring using minimally invasive procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Make Excuses for Excessive Napping and Deny Sleep Apnea?

Do people say you nap too much?
Do you make excuses such as being awake but closing your eyes just to rest them?
Do you justify naps due to your age or stress?
NOTE: This isn’t about the so-called power nap of only 20 minutes.
This is about frequent, lengthy naps that take the person away from family activities or opportunities to be productive, active or involved.
Common Excuses for Napping: Falling Asleep During the Day
“I need to lie down for my back.”
“I need to rest my feet; they’re aching from work.”
“I was awake the whole time; my eyes were just strained.”
“I was awake the whole time; I was listening to the show.”
“I got up three times overnight to use the toilet.”
“I was bored.”
“Long naps are healthy.”
Unfortunately, sometimes a spouse will support the napping, a la “Your father works hard all day. He deserves a good long nap whenever he wants.”
The napping even occurs on vacations, enough so that family members may wonder how anyone could sleep so much on a vacation.
“Wake up! Wake up to the dangers of untreated sleep apnea and recognize that excessive daytime sleepiness and the tendency to doze off easily in quiet situations during the day is a typical symptom,” says Daniel Rifkin, MD, a sleep medicine expert at the Sleep Medicine Centers of Western New York.
“Not only can the treatment of obstructive sleep apnea improve your health in so many ways, but its effect on quality of life can be astounding.
“I even had one patient that said to me, ‘Dr. Rifkin, I don’t know if I should thank you or shoot you!’
“Of course I asked why, and he said to me he now knows that he could have been a better husband, employee and even a better father if he was diagnosed with his sleep apnea sooner in life.
“He sadly recalled falling sleep after dinner almost every evening when all his children wanted to do was spend time with him. Don’t be that dad!”
What about aching joints?
Certainly, many people do have back or knee pain, or aching feet from being in bad shoes all day at work.
The solutions are to stay fully awake while treating the condition with therapeutic exercise, hotpacks, hot soaks, coldpacks, a massaging tool or stretching.
If you’re compelled to lie down or recline and close your eyes due to grogginess, even if there’s an ice pack on your knee or hotpack against your back, then you must not ignore the possibility of obstructive sleep apnea.
A fully wide-awake person who had a good night’s sleep is not going to want to go to sleep just to rest their aching feet or throbbing knee.
Stop Making Excuses for Your Naps: You Might Have Sleep Apnea!
If a body part is in pain, this will not cause drowsiness or the inability to keep one’s eyes open.
Lying down and falling asleep whenever there’s some pain is highly suspect for sleep apnea.
As for telling people you were wide awake the whole time you had your eyes closed, what’s your reason for snoring during that time?
And if repeated trips to the toilet really DID short you on sleep, then hear this: Untreated sleep apnea often causes buildup of urine overnight!
This is because the negative pressure in the thorax, caused by struggling to get air through an obstructed airway, fools cells in the heart into thinking there’s fluid retention.
These cells send a signal to the kidneys to make urine to expel the imagined fluid.
If a family member expresses concern over your excessive napping, listen to that person patiently and do not blow them off.
Keep quiet as they voice their worry, especially if they toss in some information about obstructive sleep apnea.
Your next step is to discuss this with your physician.
Dr. Rifkin is board certified in both neurology and sleep medicine. He also treats insomnia, RLS and narcolepsy.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
All the Possible Causes of Substernal Chest Pain Including Cancer

You already know that clogged coronary arteries, heart rhythm disorders and muscle strains can cause substernal chest pain, but there are causes you have no idea about. (more…)

Could Back Pain for Two Years Be Pancreatic Cancer?

Back pain that won’t go away after two years of conventional treatment may actually be due to a cause far more seious than just an irritated disc or muscle spasms.
“It is possible that back pain experienced over two years could be attributable to pancreatic cancer,” says Jordan Winter, MD, a hepato-pancreatic-biliary and oncology surgeon and Chief of the Division of Surgical Oncology at University Hospitals Cleveland Medical Center. (more…)
Staging of Pancreatic Cancer: Brief Explanation in English
Here is how pancreatic cancer, which has a very dismal prognosis, is staged — explained in a way that you will understand.
Facts About this Disease
- Five year survival rate is 8.5 percent.
- Incidence is about 12 to 13 people per 100,000 in the United States.
- There are numerous types of pancreatic cancer.
- Severity of symptoms do not necessarily correlate to the stage of this illness.
“In order to provide the most accurate prognosis for patients with pancreatic cancer, and determine the best course of therapy, we stage the disease,” says Jordan Winter, MD, a hepato-pancreatic-biliary and oncology surgeon and Chief of the Division of Surgical Oncology at University Hospitals Cleveland Medical Center. (more…)




































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}