

Chest Pain Every Day except During Exercise?

Chest pain is a very common symptom that can occur every day for benign reasons but also heart related reasons.
One condition that can cause chest pain on a daily basis is gastroesophageal reflux disease (GERD). This is chronic acid reflux.
It will feel reassuring to the person who experiences chest pain nearly every day except during exercise, making them believe that it can’t possibly be heart related.
Unexplained chest pain, however, needs to be investigated by a doctor.
It may not be heart related, but may have some other serious cause such as cancer (e.g., lung, lymphoma) or a blood clot in the lung.
- The No. 1 reason that people present to emergency rooms is chest pain.
- Most of these patients are not diagnosed with a heart problem.
“There are many factors that contribute to the burden of daily chest pain,” says Lance S. Burns, MD, emergency medicine specialist, of Legacy ER & Urgent Care, Frisco East location.
“Such include the straining of chest wall muscle fibers and irritation within the lining of the lungs.
“One should always see their physician when chest pain is a concern, either daily or intermittently.”
Dr. Burns adds that “a cardiac stress test and blood work to evaluate for potential clotting may be indicated” when standard ER tests turn up negative.
“Certainly at a minimum a chest X-ray would be a useful diagnostic tool.”
What can a chest X-ray show?
A chest X-ray can help diagnose chest pain by providing images of the heart, lungs and chest wall.
It can reveal abnormalities such as:
• Fluid accumulation around the lungs (pleural effusion) or heart (pericardial effusion).
• Enlarged heart (cardiomegaly), which may indicate heart failure.
• Lung infections or diseases, like pneumonia or bronchitis.
• Collapsed lung (pneumothorax) or pulmonary embolism.
 Dr. Burns has over 30 years of experience, and he specializes in emergency medicine as well as family medicine. For more info: Legacy ER & Urgent Care.
Dr. Burns has over 30 years of experience, and he specializes in emergency medicine as well as family medicine. For more info: Legacy ER & Urgent Care.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Angina in a 21-Year-Old: Could Be a Heart Problem?

If you’re 21 or around this age and think you might have angina, go see a cardiologist.
“Yes, any age can suffer from acute coronary insufficiency, even millennials,” says Lance S. Burns, MD, emergency medicine specialist, of Legacy ER & Urgent Care, Frisco East location.
Just what is angina?
It’s chest pain resulting from insufficient blood flow throughout the heart.
Blood flow in the heart takes place via the coronary arteries.
These arteries branch from the aorta (the largest blood vessel in the body) and are essential for maintaining the heart’s function and overall cardiovascular health.
An inadequate blood flow is usually caused by narrowing of the coronary arteries due to plaque buildup or the so-called clogging or blockages.
This narrowing, called atherosclerosis, results from the accumulation of fatty deposits, cholesterol and other substances, and this is collectively known as plaque.
Over time, these deposits can harden and restrict blood flow, leading to reduced oxygen delivery to the heart muscle.
Angina is more likely to occur during physical exertion (“stable angina”), when the oxygen demands of the heart are increased.
But not enough blood is getting through, due to the smaller diameter of the inner arteries, thanks to the plaque buildup.
This situation can actually be present in a 21-year-old. Note the image below depicting the reduced diameter due to plaque buildup.
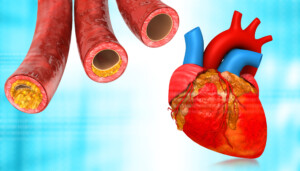
Shutterstock/Explode
Dr. Burns continues, “There are multiple factors involved with early-onset coronary syndromes.
“Genetics has a significant role. Lifestyle issues, particularly smoking and drug use (cocaine), are additional risk factors.
“In women, hormonal therapy and pregnancy are risk factors.
“Prizmental’s angina, ‘coronary spasm,’ has a higher frequency in younger, otherwise healthy individuals.”
The spasm has nothing to do with arterial blockages or heart disease, but will produce the chest pain because the spasms interfere with blood flow in the heart. This can happen in a person who’s only 21.
So though it’s very uncommon for 21-year-olds to have symptomatic heart disease, it’s certainly not unheard of in the medical world.
Dr. Burns has over 30 years of experience, and he specializes in emergency medicine as well as family medicine. For more info: Legacy ER & Urgent Care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/siam.pukkato

You Smell Like Onions Because…

A doctor explains what could make you stink like onions.
“There are multiple reasons why a person might smell like onions,” begins Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
“The first reason (which you have no control over) is genetics. You could have inherited a propensity to smell a certain way.
“Another reason you could smell like onions is that you have been eating onions – or other foods like garlic, shallots, etc. – that contain volatile sulfurous substances.
“These substances make their way into the bloodstream and by this route cause our sweat and other body fluids to smell like onions – especially in the 24-48 hours after eating them.”
You may not even know you’ve recently eaten onions in, for instance, a chicken pot pie.
Dr. Boling continues, “Even if you have not been eating onions, body sweat (especially under the arms and in the groin) can smell like onions when sweat is mixed with bacteria on the skin.”
Solutions
Dr. Boling explains, “You can limit this by showering regularly and preventing excessive sweating – by using an antiperspirant.
“A less common reason for unusual body odor is illness – for example kidney or liver disease.”

Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Wake Up Dog Tired After Feeling Great the Night Before?

Just WHAT is going on when you’re full of energy straight through the late evening but then wake up dog tired after eight hours of sleep?
Perhaps the following has happened to you many times: All day long you’re full of energy, feeling great, and even right up to the last minute before bedtime, you still feel like you have a lot of productivity left in you, but it’s time to go to bed because you want eight hours of sleep.
You sleep soundfully; the alarm goes off after eight hours, and doggone, you feel like you’ve had only four hours of sleep, and feel like you can sleep another four hours—easily.
But you absolutely must get up to begin the new day, and furthermore, you keep reading that getting more than nine hours of sleep is associated with health ailments—even exceeding eight hours has been linked to medical problems. So you drag yourself out of bed.
Strangely, within 10 minutes, you’re beginning to feel quite awake, and you accomplish another very productive day.
Even when you’ve had seven or even six hours of sleep (having to get up early for an appointment), you feel energized throughout the day and evening and never experience drowsiness or the need for even a single catnap.
Now let’s assume you don’t ingest much caffeine, if at all. You work out and are very physically fit.

Freepik.com
And you don’t have sleep apnea (a person with sleep apnea will feel drowsy throughout the day and want to take naps).
“A person could wake dead tired for a number of reasons,” begins Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
“Drinking alcohol at night can interfere with sleep and cause a person to awaken tired the next day, even if they think they slept soundly,” continues Dr. Boling. But what if you don’t drink?
“Exercising too late in the evening can also interfere with sleep – as it acts as a stimulant,” she continues.
- But what if your exercise routine was earlier in the day?
- Or what if it was one of your light-day workouts? Why does eight hours of sleep feel like only four?
Why do you feel your body needs at least two more hours of sleep, and your eyes are so heavy and groggy, as you lie there in bed, dreading having to get up for the day?
Why aren’t you one of those people who have no problem exiting their bed the moment they awaken—those enviable individuals who’ve told you that if they stay in bed once they awaken, they won’t be able to fall back asleep?
Dr. Boling offers more explanations: “Eating a heavy meal late at night can also interfere with sleep and make a person feel sluggish the next morning.” But you don’t eat heavy meals late at night, right?
“Keeping the room too warm at night might cause restless sleeping and cause a person to awaken feeling dead tired.”
And what if your room’s temperature is kept at a steady 72, and what if you’ve tried other temperatures, and you continue to feel dead tired in the morning?
“We make melatonin once the sun goes down to help us sleep at the correct time and keep our circadian clock functioning properly – it’s a chemical produced primarily in the pineal gland,” says Dr. Boling.
“Exposure to a computer or TV at night reduces melatonin production as well as stimulates a nerve pathway from the eye to parts of the brain that control hormones, body temperature and other functions that could influence the quality of sleep.”
Try to get all of your eight hours of sleep between 10 pm and 6 pm.
Yes, I know that’s utterly impossible for some people, but logistically quite feasible for others. Or shoot for 11 pm to 7 am, or midnight to 8 pm as the third option.
But the later you push bedtime back, the more you’ll throw off your circadian rhythm.
Could it be psychological?
Psychological explanation should be strongly considered. Do you feel dead tired after eight hours of sleep on the first day of your vacation at the ski resort or at the tropical island?
In fact, I’m betting that on the first day of your much-anticipated vacation in Las Vegas, Spain or with beloved extended family members only a few hundred miles away, you jumped out of bed after only five hours of sleep, as wide awake as if you’d already been up for a few hours. No need for an alarm clock.
After five or six hours you naturally awakened and were minus that awful grogginess and heavy eyes, unable to drift back into slumber.
You threw off the covers and instead of dragging yourself around, excitedly bounced about as you got ready for the day.
It’s also possible that you may not actually be asleep for as much time as you think.
Does it take a long time to fall asleep because you keep reflecting upon all of your problems or tasks for the next day?
Do you wait until mornings to organize your day and figure out what needs to be done? The anticipation of this can cause trouble falling asleep.
So even though you were in bed for eight hours, you were asleep for only five; hence, why you feel dog tired in the morning.
Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Chin Muscle Twitching: Harmless or Disease?

Has your chin been twitching lately, making you scared that you might have a neurological disease?
Before I go any further with this, I want to make sure you understand that this article is about twitching muscle fibers that are located in the chin.
There are other kinds of “twitches” that can occur about the chin, such as tics.
But I’m referring to fasciculations: the firing of muscle cells by electrochemical nerve impulses.
The face is full of muscles, and this includes the area below the surface of the chin.
Just like an eyelid might begin twitching like mad one day (yes, there are muscles there), the chin may one day begin twitching.
Do not lose sleep just because your chin is twitching.

Shutterstock/LStockStudio
“Benign muscle twitching is very common,” says Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
Dr. Boling continues, “Usually a muscle moves because we have directed it to do so, but occasionally a muscle fiber becomes overly sensitive and will move, or twitch on its own.”
Causes of Twitching Muscles in the Chin
“This can happen because a person is fatigued, not getting enough sleep, under a lot of stress, drinking too much coffee or other stimulants, overexertion or dehydration,” says Dr. Boling.

Image: Freepik.com
And just because the muscles of the chin don’t work like the muscles of your legs and feet, doesn’t mean they shouldn’t twitch from fatigue, inefficient water intake, stress or the other benign causes of fasciculations.
Dr. Boling adds: “If muscle twitching happens continuously for days or weeks, or intermittently for more than two months, then further evaluation might be indicated.
“However, most muscle twitches are completely benign and will resolve on their own.”
Do not panic if your chin (or other body part) has been twitching for weeks or even months, especially if there are no other symptoms, namely marked muscle weakness.
The longer that you have time behind the twitching with nothing ever coming of the twitching, the more reassuring this is, but in the meantime, the rule of thumb is that there’s no need to panic.
Nevertheless, a clean bill of health by a physician, after examining you for any neurological ailments, will provide enormous peace of mind.
Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/George Rudy

Can Obesity Itself Cause a Bleeding Belly Button?

There IS a link between a bleeding belly button and being obese. The situation needs prompt treatment by a doctor.
“Obesity itself does not cause a bleeding belly button, but it may contribute,” says Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
Dr. Boling explains, “The most common reason for a bleeding belly button is a skin infection of some sort – bacterial or fungal.
“We all have bacteria and fungus, but usually the skin is an effective barrier. However, dry skin can crack and allow bacteria or fungus to penetrate and take hold.”
The Obesity Factor
“Because water loss is greater for obese persons (due to greater skin surface area), morbidly obese patients have significantly drier skin (and thus a less effective barrier) as well as impaired wound healing,” says Dr. Boling.
“All of this makes getting a skin infection of the belly button more likely.
“Also, obese patients have larger skin folds and tend to sweat more profusely due to thick layers of subcutaneous fat.
“This could cause wet skin folds to rub together and become inflamed, further breaking down the barrier function of skin.”
Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Appendicitis Come and Go or What? Doctor Explains

Can on-again, off-again severe pain in your stomach be appendicitis?
“There is controversy about this even in the medical community,” says Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
“Several studies have documented both recurrent acute appendicitis as well as chronic appendicitis,” continues Dr. Boling.
“One of these studies quoted the following: The perception that acute appendicitis might subside spontaneously and re-emerge with bouts of right lower quadrant pain (so-called recurrent appendicitis) has met debate and disbelief.
“Nonetheless, 10% of patients presenting with acute appendicitis report previous similar physical findings that settled without surgery.”
What are the causes?
Dr. Boling explains, “Acute appendicitis is caused by an infection that may be preceded by the appendix becoming obstructed by a lump of feces, calcium salts or fecal debris (called fecaliths).
“There are theories as to how this could happen. Some hypothesize that the appendix might be only partially obstructed and this obstruction clears on its own or is so mild that a chronic condition ensues.
“However, the lion’s share of appendicitis is acute and requires life-saving surgery.”
So if you’ve been having abdominal or stomach pain that comes and goes, the coming and going nature does not eliminate the possibility that it’s appendicitis.
Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Inspiration GP

At What Age Do Ankles Start Swelling?

Is ankle swelling more a function of how old you are than your health?
I posed this question to Kathryn Boling, MD, a board certified family medicine practitioner with Mercy Medical Center in Baltimore, MD.
Dr. Boling explains, “This is almost an impossible question to answer, because the age at which swelling occurs has to do with the general health of the person as well as their genetic makeup.
“For example, a woman who has inherited a propensity for varicose veins who has had a few children (which has worsened this condition) might experience swelling of the legs in her 30s.
“That same woman might not have swelling until her 40s if she had remained childless.
“Also, an athletic person of 60 might never have swelling in the legs, while a very obese person in their 20s might be having constant lower extremity swelling.
“That same athletic person might have swelling if he went on a long plane trip.
“In general though, the older a person gets, the more likely that they will have some swelling.”
Another Point to Consider
The so-called sock indentations might make you think you have swelling or edema in your ankles—at least if you’ve recently had a milestone birthday such as 40 or 50.
Just because socks cause imprints of their patterns in your skin near the ankles doesn’t mean you have some kind of edema related swelling there.
If you go to a gym and make a point of looking, sooner or later you will start seeing 20-somethings walking around with the patterns of socks imprinted into the skin of their calves at varying points, including near the ankles.
This imprinting can even happen at the wrists if you’ve had a rubber band or a watch band around your wrist. It happens with the pattern of snug fitting underwear at the waist, too.
And of course, as people age, their skin loses elasticity, making it easier to “indent” from something pressing into it, especially if there’s excess body fat.
Dr. Boling diagnoses and treats a wide range of conditions from acute illnesses to chronic diseases such as diabetes and hypertension, and has 20 years’ experience with Mercy Medical Center-Baltimore.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Bell Photography 423

WHY Kids Are Scared of the Dentist; Solutions for Parents

Knowing why children are afraid of the dentist will really help you correct this problem.
“In my opinion, I believe that kids are very much influenced by their parents,” says Cyndi Blalock, DDS, owner of Cardinal Dental in St. Peters, MO.
“If their parents are afraid of the dentist, most likely the child will grow up with similar fear,” continues Dr. Blalock.
It’s simple: Children internalize their parents’ anxieties. And there are adults out there who are scared out of their wits of the dentist. This is evident in online forums. Also, why do you think there’s a such thing as “sedation dentistry”?
Dr. Blalock explains, “There have been many times that I have had a parent in the room and they themselves were so nervous that they began making scary comments about what I was doing.
“Or I told the parent that the child has a cavity, and their immediate response was, “Well, you’re getting a shot in the mouth.”
While that may be the truth, I have ways that I can numb a pediatric patient without them ever know that a shot was used to do it!
“But if the parent tells them they’re getting a shot, its an uphill battle for me to try to will over a child and convince them that I’m not going to hurt them. After all, mom said this is going to hurt!”
Parents need to choose their words carefully and not think that this is coddling their child or will make their child a wimp.
Words are powerful. If you think that kids are just overly sensitive, imagine how you’d feel (assuming you’re a woman), if your husband or mother one day said, “That dress makes you look fat.” Words…
Dr. Blalock says, “Sometimes if a child has had a previous bad medical experience such as an illness resulting in hospitalization, surgery or injury, he or she will have a harder time not being fearful of the dentist. The fear of the unknown can also contribute to it.”
Don’t act nervous even about your own upcoming dental treatment.
If your child hears you expressing your own fears about an upcoming dental appointment, don’t be surprised if this leaves an unshakeable impression.
Even if you say nothing, your child will see your body language as you sit in the waiting room, fidgeting, looking unnerved.
Though this article is mainly about why children can develop a fear of the dentist, it’s also important to hear what Dr. Blalock advises to resolve or prevent this problem.
She explains, “Encourage your child to not be fearful of the dentist. Instead of instilling fear of the dentist into your child, instill trust in them.
Most dentists really do not enjoy hurting people, contrary to how we are portrayed in the movies and in the media. Never use the word ‘shot’ to your child.”
Here are more words to avoid using: drill, scrape, poke, dig and needle. Friendlier words are: polish, make sparkle, instrument and check things out.
 The health of Dr. Blalock’s patients is a top priority at Cardinal Dental. She provides a comfortable and caring environment where she can effectively customize a dental plan to suit the needs of you and your family.
The health of Dr. Blalock’s patients is a top priority at Cardinal Dental. She provides a comfortable and caring environment where she can effectively customize a dental plan to suit the needs of you and your family.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Vitali Michkou
Can Wisdom Teeth Removal Cause Nerve Damage?

A dentist says that nerve damage can be caused by the removal of wisdom teeth.
Here is what Cyndi Blalock, DDS, explains: “Yes, it can, if the patient is built with a inferior alveolar nerve running close to the impacted wisdom tooth.”
Dr. Blalock is the owner of Cardinal Dental in St. Peters, MO.
She continues, “While this is a rare situation, it is a known complication.
“I don’t remove impacted wisdom teeth, but I do counsel my patients on the possibility of nerve damage if it appears that the roots of the wisdom teeth are close to the nerve canal.”
Nerve Damage from Wisdom Teeth Removal
Nerve damage from wisdom teeth removal can manifest as tingling or numbness in the affected area.
While such symptoms may be temporary and resolve as healing progresses, there is a risk of permanent nerve damage in some cases.
In addition to the inferior alveolar nerve, another nerve might sustain damage: the trigeminal nerve, which is one of the 12 cranial nerves — the fifth one.
In this case, the tongue would be affected – with pain, tingling or numbness.
These sensations may also involve the teeth, gums, lower lip and even the chin.
The trigeminal nerve is a major facial nerve. It has three main branches: the ophthalmic, maxillary and mandibular nerves.
These branches provide sensory information from the forehead, upper jaw and lower jaw, respectively.
The trigeminal nerve also controls muscles involved in chewing.
However, the damage from a wisdom tooth extraction is usually temporary, though this can go on for up to a few months. In rare cases of severe damage it’s permanent.
A nerve injury from root canal removal (involving either the inferior alveolar or trigeminal nerve) would cause symptoms of only sensation rather than function.
There would not be any weakness in the muscles of your tongue and lip.
Before you decide to forego having your impacted wisdom teeth removed due to fear of a nerve injury (which, remember, is usually temporary), remind yourself that making this decision could result in worse problems.
• Partially grown-in wisdom teeth that are not extracted can cause a bacterial infection.
When these teeth do not fully erupt or are only partially emerged, they create an environment where bacteria can accumulate around the gum line.
This condition, known as pericoronitis, can cause pain, swelling, and infection of the surrounding tissues. If left untreated, the infection can potentially spread and lead to more serious complications.
• Teeth that have remained non-erupted can cause a cyst – which can damage gum and bone.
These cysts, known as odontogenic cysts, form in the jawbone or surrounding gum tissue and can cause damage to both the gum and bone.
As the cyst grows, it can erode surrounding bone structures, potentially leading to pain, swelling, and further complications.
• If the teeth grow in, but are crooked, this can impair bite alignment, leading to jaw pain.
Bottom line: If your dentist advises you to have your wisdom teeth removed, have this done.
The health of Dr. Blalock’s patients is a top priority at Cardinal Dental. She provides a comfortable and caring environment where she can effectively customize a dental plan to suit the needs of you and your family.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}