

A fully functioning patient with CHF who’s medically stable, although with chronic renal insufficiency, could have acute decompensated heart failure at any time.
There are people with chronic heart failure who go dancing, bike riding, even hiking.
It’s scary to think that at any time, with seemingly no triggers, they can acutely decompensate.
This may happen even if the patient is following doctors’ orders, taking all their medications, watching sodium intake, drinking plenty of water, etc.
What causes ADHF to blow in out of the blue?
“I think it’s the teetering physiology effect — that the heart is barely holding on and the kidneys are barely holding on,” explains Mark Pool, MD, a board-certified cardiothoracic surgeon based in TX who’s been in private practice since 2011.
“And then it doesn’t take much at all to push the patient over the (physiologic) cliff,” continues Dr. Pool.
“Might be atrial fibrillation — by itself not dangerous (except for risk of stroke), but fib does slightly impair the efficiency of the pumping of blood.”
A-fib is a heart rhythm disorder, and many people with CHF do have A-fib, including undiagnosed A-fib.
Rhythm abnormalities will not always show on an eight-second EKG strip.
A person with atrial fibrillation can go days without an arrhythmia episode.
Dr. Pool continues, “So the ejection fraction might not technically reduce, but the patient may go into florid heart failure ‘all of a sudden,’ when they seemed to be getting along okay.
“For another patient, it might be a bout of diarrhea [which causes dehydration].
“For example, a patient gets dehydrated, fluid balance gets off — here comes decompensation. Doesn’t happen to everyone with low ejection fraction and diarrhea, but it is possible.
“The list goes on and on. What should normally be a day or two or feeling puny — with a ‘stomach bug’ or bronchitis or whatever — turns into a hospital stay for a patient with chronic heart failure.
“We commonly see this with elderly patients, but it happens to younger patients as well.”
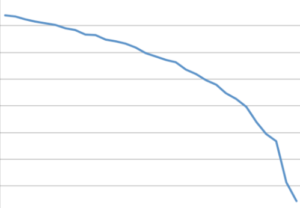
The blue line below represents chronic heart failure. It’s a steady and gradual decline over time, but where it suddenly becomes precipitous is symbolic of the onset of acute decompensation.
Unless the patient reports a lot of diarrhea or some other marked variable such as being stranded in the heat without water; ingesting a huge amount of sodium in one sitting; being on a long airline flight and having several alcoholic drinks with salty pretzels; or catching a bad cold, it will not be possible to determine the precise cause or trigger of ADHF.
In fact, acute decompensated heart failure may occur as a result of acute liver and/or kidney failure that was triggered by chronic heart failure!
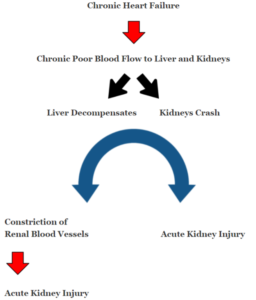
Acute kidney injury then leads to worsened cardiac function which then begins the feedback loop of cardiorenal syndrome.
As you can see, in a person with chronic HF, the pathogenesis of acute decompensated heart failure does not necessarily begin with the heart.
The liver is voracious: It demands 25 percent of cardiac output. The kidneys are right behind with 20 percent.
It’s easy to see how chronic heart failure could cause a sudden or acute decline in the function of the liver or kidneys. And these declines all play on each other, causing feedback loops of increasing deterioration.
The “at any time” concept is not a template, however. There are variables not yet understood or even known, which is why a 94-year-old with an ejection fraction of under 25 percent will be humming along through life without consequence – other than poor stamina.
And meanwhile, a 74-year-old with an EF of 30 percent will begin developing symptoms that rapidly progress to incapacitation – and be diagnosed with acute decompensated heart failure.
Nevertheless, ADHF can happen to anybody with a diagnosis of chronic HF.
Of course, it’s more likely to swoop in out of the blue for someone with an ejection fraction under 20 percent and over age 80 than in someone with an EF of 35 percent and under age 80.
Mortality rates go way up as age goes up. Treatments that may work to return a baseline function to a 70-year-old with ADHF will probably be futile for the 90-year-old.

Dr. Pool performs some of the most complicated and high-risk heart surgeries in North Texas, including redo operations and multi-valve surgery, and has performed over 3,000 major operations.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.